



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Radiology and Imaging
Volume 5, Issue 3, July 2021, Pages 12–16
Original researchOpen Access
Fast magnetic resonance arthrography of the labrum
-
Collette L. English1, MD, Fintan J. Shannon2, MD and
Diane Bergin3,*
 , MD
, MD
*Corresponding author: Professor Diane Bergin, Department of Radiology, University Hospital Galway, Newcastle Rd, Galway. Ireland. Tel.: 00353 91542626; Email: dianebergin@yahoo.com / dianebergin@hse.ie
Received 2 May 2021 Revised 11 June 2021 Accepted 17 June 2021 Published 25 June 2021
DOI: http://dx.doi.org/10.14312/2399-8172.2021-3
Copyright: © 2021 English CL, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
Research question: Short volumetric interpolated breath hold exam (VIBE) 3D gradient echo sequences are comparable to T1 spin echo (SE) sequences for evaluating the shoulder labrum using arthroscopy as a gold standard. Methods: 24 patients with suspected labral tears had magnetic resonance (MR) arthrography of the shoulder using 1.5T MR scanner. Coronal oblique 3D VIBE FS sequences were performed and reconstructed in axial and sagittal oblique planes and compared with standard T1 SE sequences. Presence and location of labral tear and rotator cuff tears were noted. Findings were correlated with surgery where available. Time to obtain T1 SE sequences versus 3D VIBE acquisition was recorded. Results: Of 24 patients, 54% had arthroscopy. Sensitivity and positive predictive value (PPV) of both T1 SE and VIBE sequences for labral tears was 92%. 100% agreement for diagnosis of labral tear by readers between both sequences was noted. Specific labral tear location was accurate in 75% for both sequences. The mean time to obtain T1 SE sequences was 13.5 mins and 7.5 minutes for 3D VIBE sequences. Conclusion: Fast MR arthrography using 3D VIBE sequences shows excellent concordance with standard T1-FS sequence for diagnosis of labral tears. With shorter acquisition time and high diagnostic sensitivity 3D VIBE sequences maybe used as an alternative to standard sequences. Level of evidence: Level III retrospective diagnostic study.
Keywords: MRI arthrography; shoulder; gradient echo sequences; labrum; 3D VIBE sequences
IntroductionTop
Magnetic resonance (MR) arthrography with intraarticular contrast is the gold standard imaging technique for evaluation of shoulder joint instability. It is of particular importance in the evaluation of labroligamentous and cartilage abnormalities [1]. Standard shoulder magnetic resonance imaging (MRI) is limited in the evaluation of the glenoid labrum because of the lack of inherent joint distension. In comparison, direct MR arthrography results in distension of the joint capsule and improved visualisation of the normal anatomy and pathology. The contrast outlines intraarticular structures and delineates labral and capsular tears. The most common indication for MR arthrography is joint instability and pain and the advantages are particularly evident in the evaluation of acute pathology in young active patients.
Standard accepted sequences used in MR arthrography include T1- weighted spin echo and fast spin echo sequences with fat suppression (T1-FS) in multiple planes. Three plane T1 imaging has been advocated as the standard shoulder arthrogram protocol [2-4]. The duration of these sequences is on average 13.5 minutes. The length of these sequences can prove difficult for patients who have experienced recent trauma of the shoulder and find it difficult to keep still for the entire duration of the study. Patients with claustrophobia also find time in the scanner challenging and sometimes intolerable.
Gradient echo sequences such as isometric volumetric interpolated breath hold examination (VIBE) are of much shorter duration and are therefore ideal for patients that find it difficult to lie still for prolonged periods. Few studies have compared the efficacy of such sequences, but initial studies show them to be as sensitive as T1W sequences in the diagnosis of rotator cuff tears [5] and labral tears [6].
The purpose of this study was to evaluate if isometric 3D VIBE sequences are comparable or better than T1-FS standard sequences in the diagnosis of shoulder labral tears using arthroscopy as gold standard.
Materials and methodsTop
This was a prospective study carried out in a single tertiary referral centre. Over a 12 month period, 24 consecutive patients with clinical instability and suspected labral tears were enrolled in the study. Patients were identified by their orthopaedic surgeon and referred for MR arthrography. Ethical approval was obtained by the local ethical committee of University Hospital Galway.
Prior to MR a dilute gadolinium solution was routinely injected into each shoulder joint. With patient consent and under fluoroscopic guidance, the glenohumeral joint was injected using an anterior approach, at the junction of the middle and lower one third of the humeral head cortex using a 22G needle. To confirm adequate position in the joint capsule 0.5ml of iodinated contrast was injected. Subsequently 8 to 12ml of 0.1ml gadolinium in 20ml of saline dilution was injected intra-articularly. The patients were subsequently transferred for MRI using a 1.5 Telsa (Siemens Espree TIM 32 x 8) MR scanner. All MR studies were performed within thirty minutes of intraarticular injection. A dedicated shoulder transmit receiver coil was used for imaging. Patients were positioned in a neutral position with the thumb pointing upwards. MR arthrography was performed using coronal oblique, axial T1-FS SE and sagittal T1 SE sequences. Coronal oblique 3D VIBE FS sequences were performed at 0.7mm slice thickness and reconstructed in the axial and sagittal oblique planes with a slice thickness of 2mm. The voxels for the VIBE acquisition were isotropic thereby allowing multiplanar reconstruction in all planes. Protocols for both sequences are summarised in Table 1.
| T1-FS sequences | VIBE sequences | |
| TR/TE | 525/ 19 | 14.4/ 6.07 |
| Flip angle | 90 | 10 |
| Band with | 100 | 200 |
| FOV phase | 100 | |
| Matrix | 192 × 256 | 256 × 256 |
| Number of slices | 20 | 96 |
| Slice thickness | 3mm | 0.7mm |
| Interslice gap | 0.6 | 0.14 |
| NEX | 1 | 1 Voxels isotropic (0.73) |
| Mean scan time | 13.5 mins | 7.5 mins (including reconstructions) |
Abbreviations: FOV: Field of view; NEX: Number of excitations.
Routine T1 and 3D VIBE sequences were reviewed on separate sittings by two radiologists with fifteen and two years’ experience in musculoskeletal radiology. The reviewers were blinded to the patient details, clinical histories and the arthroscopic findings.
Interpretation of results was done in a consensus fashion with both radiologists. Initially MRI studies with the T1W images (excluding VIBE images) were reviewed separately and then 4 weeks later the MR studies with VIBE images (and excluding T1 SE weighted images) reviewed. Images at re-review were randomized and in different order than at first review. Any disagreement in results between radiologists was reviewed and a consensus was reached.
Labral abnormalities including tear and detachment were noted. A labral tear was defined as linear or diffuse increased T1 signal in the labrum which contacted the articular surface, amorphous shape of labrum indicating tear with scar and detachment as an increase T1 signal between the labrum and glenoid.
Normal variants were diagnosed and differentiated from a labral tear including a sublabral foramen, located at the 2’o clock position and representing localized detachment of the labrum from the glenoid rim and sublabral recess located at the 12’o clock position and represents a normal recess between the superior labrum and the cartilage of the glenoid cavity.
In order to describe the location of a tear, annotation of labrum was divided into anterior, inferior, posterior and superior regions and a clock face method used to describe the extent of the tear. The anterior labrum was defined from 1 to 5 o’ clock, the inferior from 5 to 7 o’ clock, the posterior from 7 to 11 o’ clock and the superior from 11 to 1 o’ clock. The labrum was evaluated on axial, sagittal oblique and coronal oblique images.
The MR labral findings were correlated with arthroscopic results where available. Arthroscopic results were regarded as the gold standard. Surgery was performed by a single orthopaedic surgeon with twelve years experience who was aware of the MR imaging report.
The separate radiological findings of the 3D VIBE sequences were compared with those from the standard T1-FS sequences. The combined time to obtain T1 SE sequences versus 3D VIBE acquisition, including post processing time was recorded.
Analysis was performed using SPSSv20. Simple descriptive statistics such as mean and standard deviation are used for continuous data, and frequencies and percentages for categorical data. Comparisons of results of surgeries were compared using Fisher’s exact test. A p-value less than 0.05 was deemed statistically significant.
ResultsTop
A total of 24 patients (age range from 18 to 63 years, mean age 30 years) had shoulder MR arthrography and were included in the study. Of this total cohort 13 patients (54%) had subsequent arthroscopy. Only 2 patients were over 50 years. 20 patients were male and 4 were females. 11 MR arthrograms were performed on the right shoulders and 13 on the left shoulder.
At arthroscopy 92% (12 of 13) patients had labral tears at surgery. One patient had a frayed superior labrum which was considered a positive result, contributing to patient symptoms. Of these, 10 (77%) involved the anterior labrum, 5 (38%) the posterior labrum, 6 (46%) the superior labrum and 9 (69%) the inferior labrum. All 12 patients had multiple or extensive tears hence the greater number of tears after subdividing the labrum.
The sensitivity of both T1 SE and VIBE sequences for the presence of labral tears was 92% with 100% agreement between VIBE and T1 SE sequences. There was one false negative for both T1-FS and VIBE sequences which was a SLAP tear at surgery. There were no false positives for either T1 or VIBE sequences.
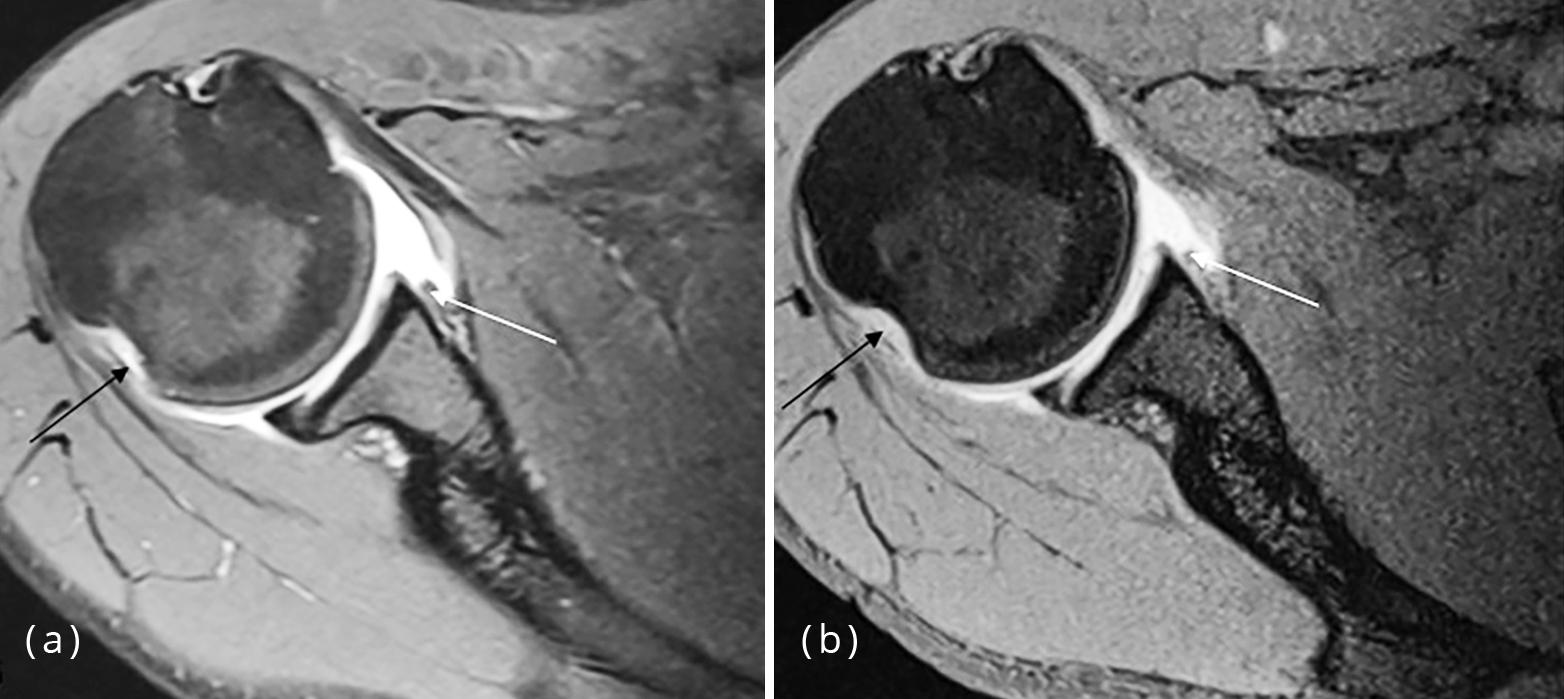
Sensitivity of both VIBE and T1W sequences for anterior labral tears was 90%, identifying 9 out of 10 tears (Figure 1). Specificity of 33% was similar for both VIBE and T1-FS.
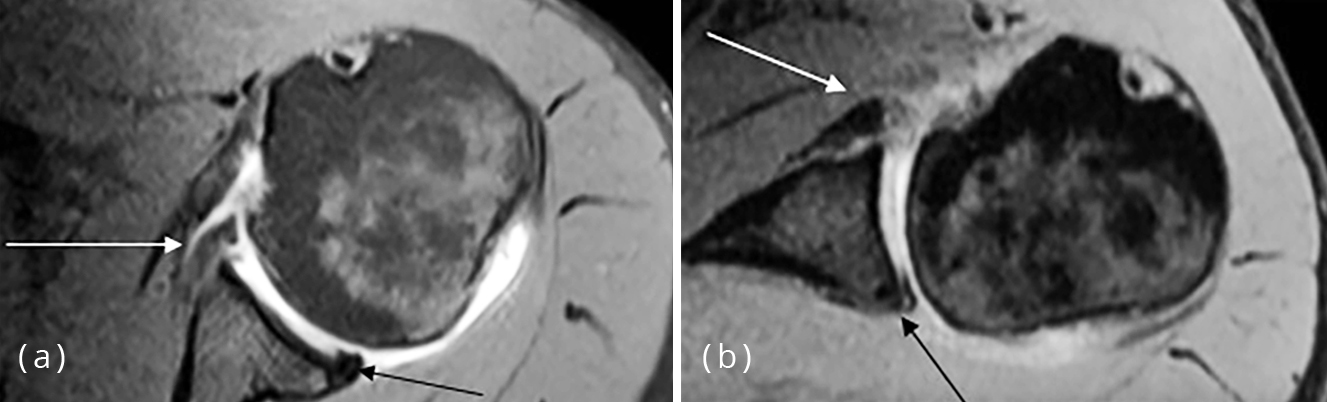
Sensitivity for posterior labral tears was 60% for VIBE sequences and 40% for T1 weighted sequences (Figure 2). There were no false positives for posterior tears.
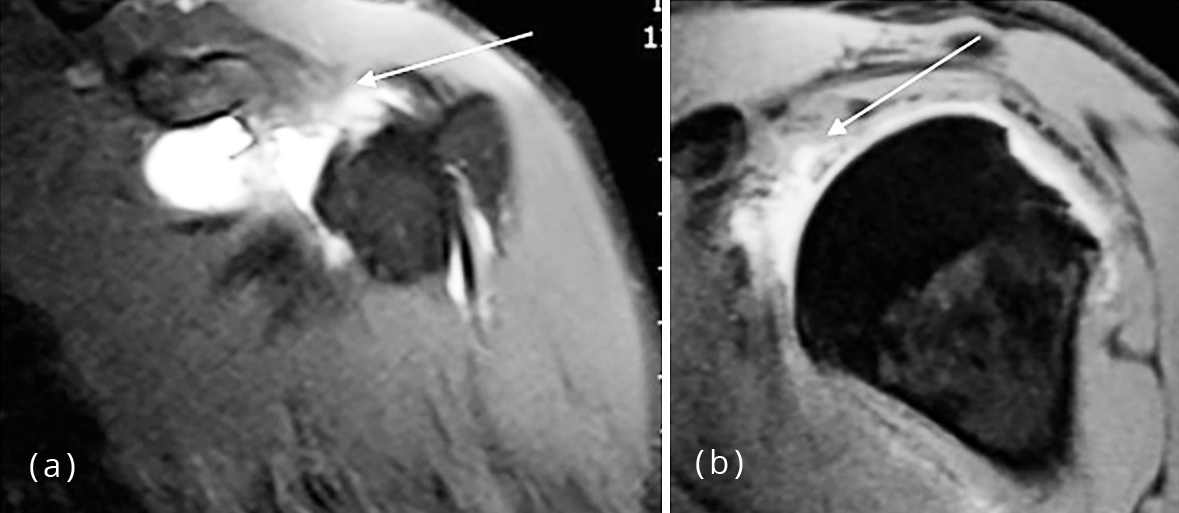
On evaluation of VIBE sequences 4 of the 6 superior labral tears were identified and confirmed at surgery (sensitivity 67%). On evaluation of T1 sequences 3 of the 6 superior labral tears were accurately identified (sensitivity 50%). Of the 7 superior labra that were normal at surgery both VIBE and T1 sequences depicted 2 tears (specificity 78%) (Figure 3). Sensitivity of VIBE and T1W sequences for inferior labral tears was 100%: identifying all 9 tears (sensitivity 100%). Of the 4 labra that did not have abnormality of the inferior labrum VIBE depicted one tear (specificity 75%) and T1W depicted 2 tears (specificity 50%). A summary of the sensitivities and specificities are presented in Table 2.
| Location in labrum | Sensitivity | Specificity | ||
| T1 % | VIBE % | TI % | VIBE % | |
| Anterior (n=10) | 90 | 90 | 33 | 33 |
| Posterior (n=5) | 40 | 60 | - | - |
| Superior (n=6) | 50 | 67 | 71 | 71 |
| Inferior (n=9) | 100 | 100 | 50 | 75 |
The mean combined acquisition time for T1 SE sequences was 13.5 minutes (range 13 to 15.5 minutes) while the mean acquisition time for 3D VIBE sequences including post processing time was 7.5 minutes (range 7 minutes to 8 minutes).
DiscussionTop
Direct MR arthrography using T1 weighted images, is the established “best” imaging technique for evaluating pathology of the shoulder labrum. The prolonged acquisition time of the T1 weighted sequences can predispose to motion artefact and reduce diagnostic accuracy of study. This is most problematic in patients with recent trauma, shoulder pain or claustrophobia who find it difficult to lie still. Often, images that are significantly degraded by movement artefact cannot be interpreted. Images obtained in a significantly faster time are potentially helpful in this patient group to ensure greater diagnostic yield of study. Faster studies also allow more efficient patient throughput in the MR scanner and greater use of imaging resources in our current environment of cost awareness.
The 3D volumetric interpolated breath hold sequence (VIBE) is a modified fast 3D gradient echo sequence with T1 weighting. It provides isotropic resolution in three dimensions, maintaining the ability to cover a wide anatomic area in a short acquisition time [7-9]. The rapid acquisition minimizes partial volume averaging and motion artefact producing high quality images [7-9]. Andrelesick et al reported VIBE sequences have a signal to noise ratio profile similar to the T1 weighted FS sequences on 1.5 and 3.0 T [10].
The shorter acquisition time and high sensitivity of gadolinium enhanced VIBE sequences are now routinely used in abdominal imaging where speed of image acquisition is even more pertinent because of consequent length of breath hold for the patient [8, 11-13].
There are few studies investigating the accuracy of the VIBE sequence in evaluating shoulder labral pathology in MR arthrography [14]. The primary concern in MR arthrography is the detection of the presence or absence of a labral tear thus allowing the referring orthopaedic surgeon to plan surgery if indicated. Palmar et al. reported sensitivities of 92% for standard T1W sequences in MR arthrography [14, 15]. To the best of our knowledge only one study has compared gradient echo sequences to T1W sequences at 1.5T for evaluation of the labrum by MR arthrography. Lee et al. [6] report sensitivity of 88% for the GRE sequences versus 64% for T1W images for the overall detection of labral tears. With sensitivities of 92% for both VIBE and T1W sequences, we have shown similar results with the VIBE sequences but greater sensitivity of T1W images in the detection of labral tears. Reported T1W sensitivities in our study for labral tears is similar to that found by Palmer et al. [14, 15].
Previous studies have reported varied sensitivities of standard T1 MR arthrography for specific labral locations: sensitivities for anteroinferior tears reported at 88% [16], anterior tears 86-95% [17] and posterior tears of 83% [18].
A recent study by Choo et al. [19] found that 3D isotropic MR arthrography may be comparable with that of conventional 2D MR arthrography in the diagnosis of both rotator cuff and labral lesions with a shorter imaging time. They did not subdivide the labrum but found overall sensitivities of 85% for 3D FSE sequences versus 83% for conventional T1W images and specificities of 80% for 3D FSE versus 83% for conventional T1W sequences in the diagnosis of labral tears.
In subdividing the labrum we found that 3D VIBE sequences were more sensitive in the diagnosis of posterior and superior labral tears compared to the T1-FS sequences. Higher sensitivity of VIBE sequences in the diagnosis of posterior labral tears was also reported by Lee et al. [6], 75% vs 25%, but not significantly different for superior labrum.
We show an equal sensitivity of the VIBE and T1W images in the detection of anterior and inferior labral tears with VIBE sequences more specific in the detection of inferior labral tears. Direct comparison of these results to previous studies, in particular Lee et al. [6] is not possible as subdivisions of the labrum were different between both studies. Despite this, overall we have shown greater sensitivities with VIBE sequences but similar specificities for the detection of anterior and inferior labral tears.
3D VIBE sequences had sensitivities and specificities that were either equal to or higher than T1W sequences for the detection of labral tears. The use of thinner slices, smaller interslice gap and therefore an increased number of slices in the VIBE images compared to the T1W sequences allowed for improved or equivalent detection of labral tears.
Gradient echo sequences can be associated with magnetic susceptibility artefacts. In patients with history of shoulder surgery VIBE sequences should be performed with care. Images should be reviewed for diagnostic quality when performed. If susceptibility artefact is limiting diagnostic quality of study alternative non gradient echo sequence with modified parameters limiting magnetic susceptibility should be considered. Of the 13 patients that underwent arthroscopy in this study two had previous surgery. Susceptibility artefact was not in the immediate vicinity of the labrum and VIBE sequences did not affect the diagnostic quality in either patient.
Considering T1-FS sequences as the gold standard imaging technique, the results show that VIBE sequences displayed excellent concordance for the presence of labral abnormalities in preoperative evaluation.
In our institution, the time of acquisition for routine T1 sequences was on average 44% longer than that of the combined VIBE sequence in a single plane and post processing time to produce alternative planar reconstructions. Reduction in scan time improves patient comfort, reduces chance of motion artefact and enhances patient throughput and MR scanner efficiency.
There were a number of limitations in the study. Firstly, the cohort was small with only 54% having subsequent surgery. Nonetheless our findings reiterate findings of prior studies that this sequence has great potential use in MR arthrography. Secondly, there was a variable amount of time between the MR arthrogram and the arthroscopy, varying from a few weeks upto 6 months, during which time further damage to, or healing of the labrum may have occurred. Another weakness is an inherent difficulty in accurately matching description of arthroscopic and radiological labral tear locations absolutely, thereby allowing possibility of under calling or overall calling pathology or integrity of labral tears at particular sites. Nonetheless, the fact that all arthroscopies were performed by the same surgeon provides greater homogeneity of surgical findings. For future studies a surgical diagrammatic map and clock of labral findings may be used to directly correlate with MR arthrography findings.
ConclusionTop
VIBE sequences for MR arthrography are as accurate and in certain cases more accurate compared to T1-FS sequences, in the diagnosis of labral tears identified at surgery. They have a definite role in patients who are at risk of movement during study and where time limitation for study is a factor. Thus, in claustrophobic patients or in patients with pain VIBE sequences should be considered. Larger studies will determine whether this sequence should be used routinely in the wider patient population where MR arthrography is planned, similar to its current application in abdominal imaging.
Conflicts of interest
Authors declare no conflict of interest.
ReferencesTop
[1]Peterson JJ. Shoulder injections. Peterson JJ, Fenton DS, Czervionke LF eds. Image Guided Musculoskeletal Interventions. 1st ed. Philadelphia, Pa: Saunders Elsevier. 2008; 9–40. ISBN 1416029052.
[2]Chaipat L, Palmer WE. Shoulder magnetic resonance imaging. Clin Sports Med. 2006; 25(3):371–386.Article Pubmed
[3]Jbara M, Chen Q, Marten P, Morcos M, Beltran J. Shoulder MR arthrography: how, why, when. Radiol Clin N Am 2005; 43(4):683–692.Article Pubmed
[4]Shankman S, Bencardino J, Beltran J. Glenohumeral instability: evaluation using MR arthrography of the shoulder. Skeletal Radiol. 1999; 28(7):365–382.Article Pubmed
[5]Vandevenne J, Vanhoenacker F, John JMM, Gelin G, Parizel PM. Fast MR arthrography using VIBE sequences to evaluate the rotator cuff. Skeletal Radiol. 2009; 38(7):699–674.Article Pubmed
[6]Lee MJ, Motamedi K, Chow K, Seeger LL. Gradient-recalled echo sequences in direct shoulder MR arthrography for evaluating the labrum. Skeletal Radiol. 2008; 37(1):19–25.Article Pubmed
[7]Bader TR, Semelka RC, Pedro MS, Armao DM, Brown MA, et al. Magnetic resonance imaging of pulmonary parenchymal disease using a modified breath-hold 3D gradient-echo technique: initial observations. J Magn Reson Imaging. 2002; 15(1):31–38.Article Pubmed
[8]Rofsky NM, Lee VS, Laub G, Pollack MA, Krinsky GA, et al. Abdominal MR imaging with volumetric interpolated breath-hold examination. Radiology. 1999; 212(3):876–884.Article Pubmed
[9]Semelka RC, Balci NC, Wilber KP, Fisher LL, Brown MA, et al. Breathhold 3D gradient-echo MR imaging of the lung parenchyma:evaluation of reproducibility of image quality in normal and preliminary observations in patients with disease. J Magn Reson Imaging. 2000; 11(2):195–200.Article Pubmed
[10]Andreisek G, Froehlich JM, Hodler J, Weishaupt D, Beutler V, et al. Direct MR arthrography at 1.5 and 3.0 T: signal dependence on gadolinium and iodine concentrations--phantom study. Radiology. 2008; 247(3):706–716.Article Pubmed
[11]Kataoka M, Ueda H, Koyama T, Umeoka S, Togashi K, et al. Contrast-enhanced volumetric interpolated breath-hold examination compared with spin-echo T1-weighted imaging of head and neck tumors. AJR Am J Roentgenol. 2005; 184(1):313–319.Article Pubmed
[12]Lauenstein TC, Goehde SC, Herborn CU, Treder W, Ruehm SG, et al. Three dimensional volumetric interpolated breath-hold MR imaging for whole-body tumor staging in less than 15 minutes: a feasibility study. AJR Am J Roentgenol. 2002; 179(2):445–449.Article Pubmed
[13]Wetzel SG, Johnson G, Tan AG, Cha S, Knopp EA, et al. Three-dimensional, T1-weighted gradient-echo imaging of the brain with a volumetric interpolated examination. AJNR Am J Neuroradiol. 2002; 23(6):995–1002.Article Pubmed
[14]Palmer WE, Brown JH, Rosenthal DI. Labral-ligamentous complex of the shoulder: evaluation with MR arthrography. Radiology. 1994; 190(3):645–651.Article Pubmed
[15]Palmer WE, Caslowitz PL. Anterior shoulder instability: diagnostic criteria determined from prospective analysis of 121 MR arthrograms. Radiology. 1995; 197(3):819–825.Article Pubmed
[16]Waldt S, Burkart A, Imhoff AB, Bruegel M, Rummeny EJ, et al. Anterior shoulder instability: accuracy of MR arthrography in the classification of anteroinferior labroligamentous injuries. Radiology. 2005; 237(2):578–583.Article Pubmed
[17]Applegate GR, Hewitt M, Snyder SJ, Watson E, Kwak S, et al. Chronic labral tears: value of magnetic resonance arthrography in evaluating the glenoid labrum and labral-bicipital complex. Arthroscopy. 2004; 20(9):959–963.Article Pubmed
[18]Tung GA, Hou DD. MR arthrography of the posterior labrocapsular complex: relationship with glenohumeral joint alignment and clinical posterior instability. AJR Am J Roentgenol. 2003; 180(2):369–375.Article Pubmed
[19]Choo HJ, Lee SJ, Kim OH, Seo SS, Kim JH. Comparison of three-dimensional isotropic T1-weighted fast spin-echo MR arthrography with two-dimensional MR arthrography of the shoulder. Radiology 2012; 262(3):921–931.Article Pubmed
 Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved