



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Modern Human Pathology
Volume 1, Issue 1, February 2016, Pages 1–5
Case reportOpen Access
Primary plasmacytoma of the lung: A case report and review of literature
-
Emily Stuppi1,*
 ,
John Lazarchick1 and
Ellen Riemer1
,
John Lazarchick1 and
Ellen Riemer1
*Corresponding author: Emily Stuppi, M.D., Department of Pathology and Laboratory Medicine, Medical University of South Carolina, 171 Ashley Avenue Suite 304, MSC 908, Charleston, SC 29425-9080, USA. Tele.: (843) 792-4229. E-mail: stuppi@musc.edu
Received 6 November 2015 Revised 11 January 2015 Accepted 20 January 2015 Published 29 January 2016
DOI: http://dx.doi.org/10.14312/2397-6845.2016-1
Copyright: © 2015 Stuppi E, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
Solitary extramedullary plasmacytomas are uncommon entities accounting for less than 5% of all plasma cell neoplasms. Primary plasmacytomas of the lung are exceedingly rare, with approximately thirty-six cases described in the modern literature. We describe a case of a primary pulmonary plasmacytoma in a 47-year-old male. A mass within the upper lobe of his right lung was incidentally discovered on computed tomography (CT) and biopsied multiple times over the course of one year with inconclusive results. Due to continued growth of the tumor, a wedge resection of the right upper lobe was performed. Histologically, normal pulmonary alveolar architecture was effaced by a dense infiltrate of inflammatory cells. These cells were predominantly monomorphic and mature plasma cells, staining positive for CD138 and negative for CD20. [R1.5] Kappa and lambda light chain in situ hybridization revealed kappa restriction, with rare scattered lambda positive reactive plasma cells. A diagnosis of primary plasmacytoma of the lung was made, pending workup for any systemic involvement by multiple myeloma. This workup revealed a normal bone marrow biopsy, a bone scan without lytic lesions, and both urine and serum protein electrophoresis devoid of abnormal protein restriction. Approximately six months later, the patient does not have evidence of residual or recurrent disease, and is being closely monitored.
Keywords: extramedullary plasmacytoma; solitary plasmacytoma; pulmonary plasmacytoma
IntroductionTop
Solitary extramedullary plasmacytomas (SEP) are malignant neoplasms of plasma cells which occur within soft tissues without evidence of systemic involvement. Together with their more common counterpart, solitary plasmacytoma of bone (SPB), they represent less than 5% of all plasma cell neoplasms [1]. They most frequently occur in the upper respiratory tract, but less often develop within other sites, including the gastrointestinal tract, liver, lymph nodes, skin, central nervous system, and lung [2]. Primary plasmacytomas of the lung are exceedingly rare, with approximately 36 confirmed cases described in the modern literature [3, 30]. As such, there is scant data regarding prognosis and risk of progression to multiple myeloma that is specific to these pulmonary lesions. Here we report a case of a primary pulmonary plasmacytoma followed by a brief review of the literature.
Case presentationTop
A 47-year-old Caucasian man presented to the Medical University of South Carolina (MUSC) with shortness of breath and fatigue in December 2013. He was jaundiced on physical exam with a total bilirubin of 5.5 mg/dl (direct bilirubin of 2.4 mg/dl) and anemic with a hemoglobin of 6.3 g/dl. The total protein was 8.2 g/dl, with a pattern suggestive of an inflammatory process. He was initially believed to have an autoimmune hemolytic anemia, due to a positive direct anti-globulin test (DAT) and decreased haptoglobin (26 mg/dl), however his lactate dehydrogenase (LDH) was within normal limits, and he did not improve with prednisone treatment. A bone marrow aspirate and biopsy revealed an erythroid dysplasia and a hypercellular marrow (80% cellularity), with no discrete blast population identified by flow cytometry. The bone marrow biopsy was reported as refractory cytopenia with unilineage dysplasia (RCUD). Due to concern for myelodysplastic syndrome versus other causes of morphologic atypia, the patient was referred to the hematology/oncology service, who discovered during their initial interview that he was a heavy drinker. He had no vitamin deficiencies, therefore they attributed his erythroid dysplasia to alcohol consumption and advised the patient to discontinue drinking. He complied and his anemia improved.
However, during the course of this workup, it was discovered on computed tomography (CT) that the patient had a 1.1 cm nodular density in the upper lobe of his right lung. A core biopsy was attempted shortly thereafter, which revealed benign lung parenchyma with granulomatous inflammation. Grocott’s methenamine silver (GMS) stain was negative for fungus, and auramine rhodamine (AR) stain was negative for mycobacterial organisms. A second biopsy was attempted four months later with identical results. A third biopsy performed in November 2014, eleven months after the first attempt, was predominantly blood and inadequate for evaluation. Coexisting cytology specimens for these three core biopsies were concordant, consisting of granulomatous inflammation, macrophages, and bronchial epithelial cells, with no evidence of malignant cells. During these eleven months, the pulmonary nodule tripled in size. Cultures for acid fast bacilli and fungi remained negative. Due to continued growth of the mass and concern for malignancy, a wedge resection was performed in January 2015 and at that time the true nature of the tumor was revealed on histology.
ResultsTop
Gross examination revealed a 10x5x3cm red-purple lung wedge containing a 3x3x2.5cm tan-white firm and poorly delineated mass. Microscopic examination displayed infiltration and effacement of normal pulmonary architecture by a population of predominantly monomorphic and mature plasma cells, with eccentric oval-shaped nuclei and clumped chromatin. The neoplastic cells were CD138 positive with kappa light chain restriction demonstrated on in situ hybridization (Figure 1). These cells were negative for CD20, which stained scant benign extra-lesional B lymphocytes, arguing against a diagnosis of lymphoplasmacytic lymphoma.
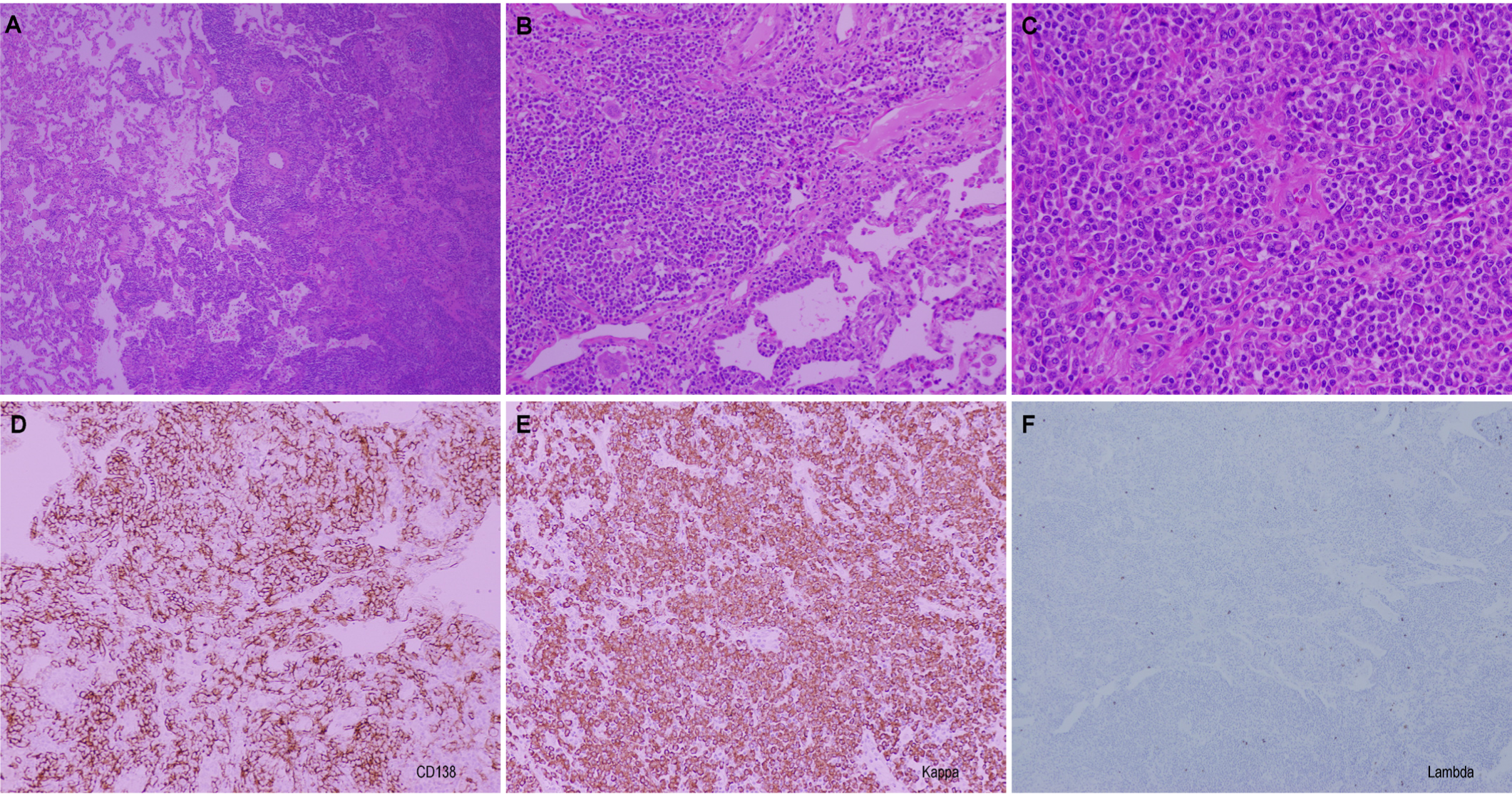
On the periphery of the lesion, the neoplastic cells extended along alveolar septal walls and showed cuffing around small vessels and bronchovascular bundles, with numerous non-caseating granulomas also present in these areas. Additionally present was a brisk population of non-neoplastic and reactive benign CD3 positive T lymphocytes which demonstrated the normal CD4 to CD8 ratio. Foreign body giant cells were numerous throughout. Congo red stain for amyloid was negative. The vast majority of the plasma cells were kappa positive, with only very scant solitary plasma cells showing lambda positivity, consistent with a plasmacytoma. Flow cytometry was not performed in this case, as a hematologic malignancy was not suspected prior to fixation of the wedge resection in formalin. The surgical pathology report was signed out as an extramedullary plasmacytoma of the lung, with kappa-positive light chain restriction.
Before the diagnosis of solitary extramedullary plasmacytoma could be confirmed, the patient underwent positron emission tomography/ computed tomography (PET/CT) in February 2015, which failed to show additional areas of disease. There was also no evidence for residual involvement at the site of resection. The patient’s serum protein electrophoresis, serum immunofixation electrophoresis, and urine protein electrophoresis did not show evidence of a monoclonal (M) protein. The ratio of kappa to lambda serum free light chains was within the normal range. A bone marrow aspiration and biopsy performed in February 2015 revealed a mildly hypocellular bone marrow with maturing trilineage hematopoiesis. There was no morphologic or immunophenotypic evidence for a monoclonal plasma cell neoplasm. Concurrent cytogenetic and fluorescence in situ hybridization (FISH) studies disclosed a normal karyotype with no aberrations.
Solitary extramedullary plasmacytomas (SEP) behave in a biologically distinct manner, although they appear histologically identical to the plasma cells seen in multiple myeloma (MM) [31]. Generally patients with SEP, in the absence of development of MM during the follow up period, outlive patients with MM by many years [32]. Unlike MM, many SEP are non-secretory, as a monoclonal (M) protein is detected in the serum of 25-50% of cases [12, 28]. In addition, the serum concentration of this M protein is usually lower than that seen in MM [23], and the persistence or increase of a monoclonal gammopathy following treatment may suggest systemic disease [25].
Progression to MM is a definite risk, although there is some debate on the frequency of such transformations, and the majority of this data comes from cases of solitary plasmacytoma of bone rather than extraosseous neoplasms [33-35]. A recent study by Katodritou et al examined 97 patients with plasmacytomas, including both SEP and SPB, and discovered approximately 25% (24/97) progressed to MM [36]. Kilciksiz et al suggested that patients with SEP have a relatively low risk of progression to MM compared with SPB patients [37]. Of the 80 patients they reviewed, 57 had SPB and 23 had SEP. A total of 25 patients developed MM (31%), and 21 of those were in the SPB group [31]. Therefore, only 4 patients of the 23 with SEP developed MM (17%) compared with 37% of patients with SPB [31]. These statistics are comparable to an earlier study conducted by Meis et al, who found that 36% of patients with SPB developed MM, compared with 23% of patients with SEP, in an average of 39 and 23 months, respectively [32]. The authors concluded that there were histologic features which might help predict biological behavior and the development of MM from SEP, including immature nuclei and prominent nucleoli, however these were encouraged to be considered in the context of radiographic and laboratory data [32].
There has not been a comprehensive review of the literature for primary pulmonary plasmacytomas (PPP) since Koss et al. in 1998 [15], who reviewed a total of 19 cases of PPP. Since then, 36 cases have been published (Table 1) which have been verified by IHC or detection of an M protein. As with prior reviews, [11, 15] cases which were not verified by IHC or did not have an associated monoclonal gammopathy were not included in this current evaluation.
| Author/Year | Age/Gender | Symptoms | Radiographic | M protein | Treatment | Follow-up |
| Robson 1959 [3] | 48 F | Cough, night sweats, chest pain | RLL opacity | Yes | Lobectomy Radiation |
10 mo: plasmacytoma of stomach 24 mo: developed MM 25 mo: DT |
| Kernen 1966 [4] | 67 M | None | L hilar mass, enlarged hilar LNs | Yes | Lobectomy Radiation |
3.5 mo: DT, MM diagnosed at autopsy |
| Wile 1976 [5] | 40 M | Fever, cough | LUL and LLL mass | Yes | Pneumonectomy | N/A |
| Baroni 1977 [6] | 14 M | Fever, weight loss | RUL mass | Yes (IgG kappa) | Lobectomy Chemo |
22 mos: A&W |
| Amin 1985 [7] | 63 M | Cough, SOB, hemoptysis | RUL mass | No | Radiation | 6 mo: dev. MM 12 mo: DU |
| Amin 1985 [7] | 72 F | Chest pain, SOB | LLL lesion | No | Lobectomy Radiation |
14 mo: developed MM 24 mo: DT |
| Amin 1985 [7] | 66 F | Cough | RUL mass | Yes | Radiation | 16 mo: developed MM 47 mo: DT |
| Roikjaer 1986 [8] | 65 F | None | LUL mass | No | Lobectomy Chemo |
2.5 yr: local recurrence (resected) 4 yr: A&W |
| Morinaga 1987 [9] | 54 F | None | LLL mass, calcified hilar LNs | Yes (IgG kappa) | Lobectomy | 6 mo: A&W |
| Kazzazz 1992 [10] | 60 M | None | R lung peripheral mass | No | Lobectomy | 9 yr: A&W |
| Nonomura 1992 [11] | 55 F | None | RUL mass | No | Lobectomy | 12 mo: A&W |
| Joseph 1993 [12] | 79 M | None | R hilar mass | Yes (IgG lambda) | Lobectomy | 12 mo: A&W |
| Egashira 1995 [13] | 50 M | None | R hilar mass | No | Lobectomy | N/A |
| Husain 1996 [14] | 70 F | None | LUL mass | No | Lobectomy | 3 yr: developed MM |
| Koss 1998 [15] | 50 M | Asthma | R hilar mass | No | Pneumonectomy | 18 yr: plasmacytoma of R ulna 20 yr: DU (MI) |
| Koss 1998 [15] | 53 M | Cough | L hilar mass | No | Lobectomy | 21 yr: DU |
| Koss 1998 [15] | 73 F | Phlebitis | RLL mass | Yes (IgG kappa) | Lobectomy | 28 mo: DT-plasmacytoma of mediastinal and abdominal LNs |
| Koss 1998 [15] | 54 F | Cough, dyspnea, hemoptysis | Unknown | No | Pneumonectomy | 36 mo: A&W |
| Koss 1998 [15] | 55 M | None | R lung mass | No | Pneumonectomy | 4 days: DT – plasmacytoma of mediastinal and paraaortic LNs, within liver |
| Piard 1998 [16] | 70 M | Dyspnea, wheezing | L hilar mass, calcified L hilar LN | No | Lobectomy | 1 yr: A&W |
| Horiuchi 1998 [17] | 45 F | Fever, cough, dyspnea | RLL and LLL infiltrates | Yes (IgA kappa) | Chemo | 16 cycles chemo: A&W |
| Chen 1998 [18] | 58 F | Cough, dyspnea | RML and LLL opacities | Yes (IgA lambda) | Radiation Chemo |
2 yr: A&W |
| Lazarevic 2001 [19] | 65 M | Malaise, weight loss, cough | LLL, RLL, and RML opacities | No | Chemo | 5 yr: A&W |
| Wise 2001 [20] | 65 M | None | R hilar mass | Yes (IgG kappa) | Lobectomy | 15 mo: A&W |
| Edelstein 2004 [21] | 47 M | Cough, wheezing, SOB | L mainstem bronchus mass | No | Rigid bronchoscopy, removed piecemeal | 8 mo: A&W |
| Marisavljevic 2005 [22] | 56 M | Cough, pain, weight loss | RUL mass | No | Radiation Chemo Lobectomy |
4 yr: A&W |
| Niitsu 2005 [23] | 71 F | None | RML mass | Yes (IgG lambda) | Chemo | 3 cycles chemo: A&W |
| Kaneko 2005 [24] | 61 F | Hemoptysis | RUL mass | Yes (IgM lambda) | Chemo | 28 mo: A&W |
| Chang 2006 [25] | 72 M | Cough | RLL lesion | Yes (IgG lambda) | Lobectomy | 10 mo: A&W |
| Shaikh 2008 [26] | 55 F | Chest pain, anorexia, cough, SOB | R lung mass | Yes | Radiation | 6 mo: A&W |
| Montero 2009 [27] | 59 M | Hemoptysis, asthma | R hilar mass, enlarged subcarinal LNs | No | Lobectomy Radiation |
10 yr: A&W |
| Montero 2009 [27] | 64 M | Fever, weight loss | RUL mass | Yes (IgG kappa) | Radiation | 15 yr: A&W |
| Montero 2009 [27] | 56 M | Hemoptysis | RUL mass | Yes (IgA kappa) | Radiation Chemo |
3 cycles chemo: DT |
| Mohammad 2010 [28] | 60 F | Dyspnea, cough | Bilateral alveolar consolidation | Yes | Chemo | 4 mo: A&W |
| Kim 2012 [29] | 26 F | Cough | RLL, LLL lesions | No | Chemo | 4 mo: A&W |
| Ujiie 2012 [30] | 43 M | None | RUL mass | No | Lobectomy | 3 mo: recurrence RML, resected 6 mo: A&W |
Abbreviations: M= male; F= female; R= right; L= left; RUL= right upper lobe; RML= right middle lobe; RLL= right lower lobe; LLL= left lower lobe; LUL= left upper lobe; mo= month(s); yr= year(s); DT= died from tumor; DU= died of unrelated causes; A&W= alive and well; MM= multiple myeloma; LN= lymph node; SOB= shortness of breath.
Of the 37 cases of PPP, the mean and median ages at diagnosis were 57 and 58, respectively, consistent with prior reviews (Table 2) [15]. This includes 21 men and 16 women, a fairly even ratio of 1.3:1, which is different from the male predilection seen with extramedullary plasmacytomas of other sites [32]. An M protein was discovered at diagnosis in 18 patients (48.6%). Of these patients, only 3 (16.6%) developed MM during the follow up period. An additional 3 patients who did not have monoclonal gammopathy at presentation developed MM at a later stage, bringing the total incidence of progression to MM to 16% (6/37). However, the follow-up period varied widely for these cases (from 4 days to 20 years), and 2 patients had no available follow-up data.
| Characteristic | No. of patients (Total=37) |
| Male | 21 |
| Female | 16 |
| Age | |
| 14-40 | 3 |
| 41-60 | 20 |
| 61-80 | 14 |
| M protein present | 18 |
| Multiple myeloma | 6 |
These numbers suggest that having an M protein at diagnosis does not have a clear association with the later development of MM. The level of monoclonal protein within the serum was not reported in all cases, therefore we were not able to determine whether having a higher level of monoclonal gammopathy would confer a greater risk for either tumor recurrence or progression into MM.
Treatment depended on the time of diagnosis. A common theme among these thirty-seven cases was the difficulty and delay in making the diagnosis. Many of these cases were not diagnosed until after surgical resection had been performed, and this served as the main form of treatment. In other cases, the diagnosis was made on a biopsy specimen, and radiotherapy and/or chemotherapy was administered.
Prognostic data is limited due to the extreme range in follow-up time period, with two cases having no follow-up and a range of 4 days to 20 years for the rest. There were 11 cases with a 6 month or less period of follow-up at the time of publication. Of these, 7 were alive and well [9, 15, 23, 26, 28-30], 2 died of their tumor [15, 27], and 2 developed MM [4, 7]. One of the patients described as alive and well did develop a recurrence at 3 months, which was surgically resected and the patient was disease free at 6 months [30].
ConclusionTop
In our case, the patient’s PPP appears to have been successfully treated by surgical resection. He continues to be monitored for recurrence and the development of multiple myeloma, but remains disease free after 10 months.
Conflicts of interest
Authors declare no conflicts of interest.
ReferencesTop
[1]Weber DM. Solitary bone and extramedullary plasmacytoma. Hematology Am Soc Hematol Educ Program. 2005(1):373–376.Article Pubmed
[2]Wiltshaw E. The natural history of extramedullary plasmacytoma and its relation to solitary myeloma of bone and myelomatosis. Medicine (Baltimore). 1976; 55(3): 217–238.Article Pubmed
[3]Robson AO, Knudsen A. Plasmacytoma of the lung and stomach. Br J Dis Chest. 1959; 53(1):62–67.Pubmed
[4]Kernen JA, Meyer BW. Malignant plasmacytoma of the lung with metastases. J Thorac Cardiovasc Surg. 1966; 51(5):739–744.Pubmed
[5]Wile A, Olinger G, Peter JB, Dornfeld L. Solitary intraparenchymal pulmonary plasmacytoma associated with production of an M-protein: report of a case. Cancer. 1976; 37(5):2338–2342.Article Pubmed
[6]Baroni CD, Mineo TC, Ricci C, Guarino S, Mandelli F. Solitary secretory plasmacytoma of the lung in a 14-year-old boy. Cancer. 1977; 40(5):2329–2332.Article Pubmed
[7]Amin R. Extramedullary plasmacytoma of the lung. Cancer. 1985; 56(1):152–156.Article Pubmed
[8]Roikjaer O, Thomsen JK. Plasmacytoma of the lung. A case report describing two tumors of different immunologic type in a single patient. Cancer. 1986; 58(12):2671–2674.Article Pubmed
[9]Morinaga S, Watanabe H, et al. Plasmacytoma of the lung associated with nodular deposits of immunoglobulin. Am J Surg Pathol. 1987; 11(12):989–995.Pubmed
[10]Kazzazz B, Dewar A, Corrin B. An unusual pulmonary plasmacytoma. Histopathology 1992; 21(3): 285–287.Article Pubmed
[11]Nonomura A, Mizukami Y, Shimizu J, Oda M, Watanabe Y, et al. Primary extramedullary plasmacytoma of the lung. Intern Med. 1992; 31(12): 1396– 1400.Article Pubmed
[12]Joseph G, Pandit M, Korfhage L. Primary pulmonary plasmacytoma. Cancer. 1993; 71(3): 721–724.Article Pubmed
[13]Egashira K, Hirakata K, Nakata H, Kawanami S, Mitsudomi T, et al. CT and MRI manifestations of primary pulmonary plasmacytoma. Clin Imaging. 1995; 19(1):17–19.Article Pubmed
[14]Husain M, Nguyen GK. Primary pulmonary plasmacytoma diagnosed by transthoracic needle aspiration cytology and immunocytochemistry. Acta Cytol. 1996; 40(3): 622–624.Pubmed
[15]Koss MN, Hochholzer L, Moran CA, Frizzera G. Pulmonary plasmacytomas: a clinicopathologic and immunohistochemical study of five cases. Ann Diagn Pathol. 1998; 2(1):1–11.Pubmed
[16]Piard F, Yaziji N, Jarry O, Assem M, Martin L, et al. Solitary plasmacytoma of the lung with light chain extracellular deposits: a case report and review of the literature. Histopathology. 1998; 32(4):356–361.Article Pubmed
[17]Horiuchi T, Hirokawa M, Oyama Y, Kitabayashi A, Satoh K, et al. Diffuse pulmonary infiltrates as a roentgenographic manifestation of primary pulmonary plasmacytoma. Am J Med. 1998; 105(1):72–74.Article Pubmed
[18]Chen KY, Wu HD, Chang YL, Shih JY, Yang PC. Primary pulmonary plasmacytoma with lobar consolidation: an unusual presentation. J Formos Med Assoc. 1998; 97(7):507–510.Pubmed
[19]Lazarevic V, Cemerikic-Martinovic V, Suvajdzic N, Subotic D, Colovic M. Diffuse pulmonary plasmacytoma of the lung. Haematologia. 2001; 31(2):161–165.Article Pubmed
[20]Wise JN, Schaefer RF, et al. Primary pulmonary plasmacytoma: a case report. Chest. 2001; 120(4): 1405– 1407.Pubmed
[21]Edelstein E, Gal AA, Mann KP, Miller JI Jr, Mansour KA. Primary solitary endobronchial plasmacytoma. Ann Thorac Surg. 2004; 78(4):1448–1449.Article Pubmed
[22]Marisavljevic D, Markovic O, Cemerkic-Martinovic V, Ponomarev D. Plasmacytoma of the lung: an indolent disease resistant to conventional myeloma treatment: report of a case. Med Oncol. 2005; 22(2):207–210.Article Pubmed
[23]Niitsu N, Kohri M, Hayama M, Nakamine H, Nakamura N, et al. Primary pulmonary plasmacytoma involving bilateral lungs and marked hypergammaglobulinemia: differentiation from extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue. Leuk Res. 2005; 29(11):1361–1364.Article Pubmed
[24]Kaneko Y, Satoh H, Haraguchi N, Imagawa S, Sekizawa K. Radiologic findings in primary pulmonary plasmacytoma. J Thorac Imaging. 2005; 20(1):53–54.Article Pubmed
[25]Chang CC, Chang YL, Lee LN, Lee YC. Primary pulmonary plasmacytoma with immunoglobulin G/lambda light chain monoclonal gammopathy. J Thorac Cardiovasc Surg. 2006; 132(4):984–985.Article Pubmed
[26]Shaikh G, Sehgal R, Mehrishi A, Karnik A. Primary pulmonary plasmacytoma. J Clin Oncol. 2008; 26(18):3089–3091.Article Pubmed
[27]Montero C, Souto A, Vidal I, Fernández Mdel M, Blanco M, et al. Three cases of primary pulmonary plasmacytoma. Arch Bronconeumol. 2009; 45(11):564–566.Article Pubmed
[28]Mohammad Taheri Z, Mohammadi F, Karbasi M, Seyfollahi L, Kahkoei S, et al. Primary pulmonary plasmacytoma with diffuse alveolar consolidation: a case report. Patholog Res Int. 2010; 2010:463465.Article Pubmed
[29]Kim SH, Kim TH, Sohn JW, Yoon HJ, Shin DH, et al. Primary pulmonary plasmacytoma presenting as multiple lung nodules. Korean J Intern Med. 2012; 27(1):111–113.Article Pubmed
[30]Ujiie H, Okada D, Nakajima Y, Yoshino N, Akiyama H. A case of primary solitary pulmonary plasmacytoma. Ann Thorac Cardiovasc Surg. 2012; 18(3):239–242.Article Pubmed
[31]Kremer M, Ott G, Nathrath M, Specht K, Stecker K, et al. Primary extramedullary plasmacytoma and multiple myeloma: phenotypic differences revealed by immunohistochemical analysis. J Pathol. 2005; 205(1):92–101.Article Pubmed
[32]Meis JM, Butler JJ, Osborne BM, Ordóñez NG. Solitary plasmacytomas of bone and extramedullary plasmacytomas. A clinicopathologic and immunohistochemical study. Cancer. 1987; 59(8):1475–1485.Article Pubmed
[33]Pavithran K, Doval DC, Rao CR, Bapsy PP, Anantha N. Pediatric solitary plasmacytoma. Acta Oncol. 1997; 36(1):83–84.Pubmed
[34]Frassica DA, Frassica FJ, Schray MF, Sim FH, Kyle RA. Solitary plasmacytoma of bone: Mayo Clinic experience. Int J Radiat Oncol Biol Phys. 1989; 16(1):43–48.Article Pubmed
[35]Liebross RH, Ha CS, Cox JD, Weber D, Delasalle K, et al. Clinical course of solitary extramedullary plasmacytoma. Radiother Oncol. 1999; 52(3):245–249.Article Pubmed
[36]Katodritou E, Terpos E, Symeonidis AS, Pouli A, Kelaidi C, et al. Clinical features, outcome, and prognostic factors for survival and evolution to multiple myeloma of solitary plasmacytomas: a report of the Greek myeloma study group in 97 patients. Am J Hematol. 2014; 89(80):803–808.Article Pubmed
[37]Kilciksiz S, Celik OK, Pak Y, Demiral AN, Pehlivan M, et al. Clinical and prognostic features of plasmacytomas: a multicenter study of Turkish Oncology Group-Sarcoma Working Party. Am J Hematol. 2008; 83(9):702–707.Article Pubmed
[38]Kennedy JD, Kneafsey DV. Two cases of plasmacytoma of the lower respiratory tract. Thorax. 1959; 14:353–355.Article Pubmed
[39]Gordon J, Walker G. Plasmacytoma of the lung. Arch Pathol. 1944; 37:222–224.
[40]Kinare SG, Parulkar GB, Panday SR, Sen PK. Extensive ossification in a pulmonary plasmacytoma. Thorax. 1965; 20:206–210.Article Pubmed
[41]Kilburn KH, Schmidt AM. Intrathoracic plasmacytoma; report of a case and review of the literature. Arch Intern Med. 1960; 106:802–809.Pubmed
 Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved