



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Neurology and Therapeutics
Volume 2, Issue 3, April 2016, Pages 8–14
Case reportOpen Access
Specific work integration program with a patient with traumatic brain injury
-
Ciampa MA1,3,*
 ,
Roca M1,2,3,4,
Torralva T1,2,3,
Lischinsky A1,
Manes F1,2,3 and
Camino J1
,
Roca M1,2,3,4,
Torralva T1,2,3,
Lischinsky A1,
Manes F1,2,3 and
Camino J1
*Corresponding author: Ciampa MA, OTD, Neuropsychology Research Laboratory, Institute of Cognitive Neurology (INECO), Buenos Aires, Argentina. E-mail: aciampa@ineco.org.ar
Received 22 December 2015 Revised 3 March 2016 Accepted 15 March 2016 Published 24 March 2016
DOI: http://dx.doi.org/10.14312/2397-1304.2016-3
Copyright: © 2016 Ciampa MA, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
Introduction: Traumatic brain injury (TBI) is one of the principal causes of disability among young adults. It can lead to physical, behavioural and cognitive impairments that affect functional performance, interpersonal relationships, social participation and work reintegration. Return to work is one of the main concerns with patients who have TBI. This depends on several aspects due to the complexity of the skills involved; and their interaction with the client´s impairment. Objective: We report the case of a Specific Work Integration Program in a patient with TBI. Methods: Mr. JC, 30-year-old patient, suffered a TBI in a car accident. The Specific Work Training Program described, consisted of different stages: assessment, interview and training. Specific questionnaires were designed, according to the patient´s skills and work requirements. Based on the data collected, particular goals were established and intervention strategies were developed. Results: Through work samples, it was possible to identify achievements in the following items: Supervision acceptance, security, tools identification, decision making and pace. Furthermore, a progressive improvement was observed in the number of tasks performed. Conclusions: The development of a specific program that involves an objective assessment of the workstation, as well as structured questionnaires, helps identify real limitations at the workplace.
Keywords: traumatic brain injury; return to work; work reintegration; job performance; occupational therapy; rehabilitation
IntroductionTop
Traumatic brain injury (TBI) is one of the principal causes of disability among young adults. It can lead to physical, behavioural and cognitive impairments that affect their functional performance, interpersonal relationships, social participation and work reintegration [1, 2]. Return to work is one of the main concerns in regard to rehabilitating patients with TBI. It depends on several aspects due to the complexity of the skills involved; and their interaction with the client´s impairment [3]. M.R. Benedictus & col. [4] have established, with a longitudinal study, that the principal difficulties people with TBI may have are firstly, cognitive, then behavioural, social, and lastly, physical affecting their return to work. The application of specific work training programs is vital, because if they are not applied, people with cognitive and behavioural impairments may not develop any kind of productive activities. Patients do not receive appropriate treatment, particularly regarding work reintegration, or they go to institutions in which interventions are not tailored and their particular needs are not fulfilled.
When working with people who have suffered a brain injury, it is of vital importance that they acquire a meaningful occupation, as this helps with the performance of productive activities [5]. It not only promotes motivation and a higher self-esteem, but also provides the opportunity to interact with others in a normalised environment. R. Sjöström et al. [6] demonstrating that people consider work an important component of life.
Even though statistics in Argentina are not available, studies in Great Britain estimate that only 40% of people with TBI return to work [7]. The authors outline the economic impact this may have on a country, emphasising the cost-benefit that work reintegration of people with disabilities implies.
Several studies have investigated the different factors that facilitate or limit work reintegration in people with TBI. For example, M. Schönberger & col. [8] have identified the importance of age, education, previous work experience, injury severity, mood, cognition and behavioural changes as determinants for functionality and employment.
Recently, Bonneterre et al. [9] provided evidence of the importance of vocational programs in the facilitation of the return to work (RTW) in regard to persons who had suffered a TBI. In particular, they described the usefulness of the personalised service of accompaniment and follow up to employment (SPASE) and report the factors associated with return to work (RTW) success at short and at medium term.
Even if many authors have pointed out the importance of designing a personally tailored treatment, according the needs of each patient [6], no further studies have assessed the utility of specific work integration programs in patients with TBI, nor have they provided a detailed description of the steps to follow or the type of professionals who should be involved within the program.
The objective of the present study is to describe the development of a Specific Work Training Program that can be used with people who had brain injuries. The program is based on an exhaustive analysis of the person´s interests and capacities, and as a result, the person would have a better chance of successfully integrating into a competitive job.
MethodsTop
Case description
Mr. JC’s case. He is 30-years-old, and suffered a TBI due to a car accident in 2002. He entered the intensive care unit immediately, presenting intracranial hypertension and several complications. The lesions shown in the initial CT head scan were predominantly in the frontal and temporal lobes. There weren’t any major extra cranial injuries. He stayed in a coma for a period of 33 days (Glasgow Coma Scale = 3) [10]. Furthermore, he presented with a post-traumatic amnesia that led him to have no memory of anything that had happened 4 months prior to his accident. He also presented with seizures, which stopped after receiving anticonvulsant medication. As another sequelae, olfactory problems had been identified.
After 60 days, he was able to open his eyes. In the next three months, an inpatient rehabilitation program had been implemented; Mr JC soon began to walk and speak, presenting anomies and paraphasia. Afterwards, he stayed at his parents’ house until March, after which he went back to the city to live on his own, receiving help from his aunt and a housekeeper. There was no decreased interaction with his friends or family reported.
Respecting Mr. JC´s previous experience, prior to the TBI, he studied Biological Sciences, and in terms of productive activities, he had worked as a sales assistant in a shop, as a helper in a Vet Hospital and assisted a Ranger during a whole season in a nature reserve.
After the TBI, he went back to study the same subject, failing to pursue to the subject in the same year. Then, he took a vocational orientation and began to study for a Bachelor in Biodiversity Handling, Management and Conservation. In respect to the work field, he had done an internship in a natural park without any professional intervention. His main responsibilities involved the maintenance and monitoring of the area and guiding the visitors along the path. Mr. J was dismissed in the after 15 days. The reasons for the dismissal from the job were related to social abilities and personal interaction problems, making this a failure experience, thus necessitating a work rehabilitation program.
In August, 2009, he started treatment at the Institute of Cognitive Neurology (INECO). INECO is a Rehabilitation Institute where psychologists, neuropsychologists, OT, speech therapists and physiotherapists work together with physicians to integrate the rehabilitative physical, cognitive and behavioural consequences in brain damaged patients.
Neuropsychological profile and mood symptoms at treatment initiation
JC complained of cognitive impairments due to his TBI including attention deficits, short term memory and word finding problems. He underwent a complete cognitive assessment, in which a moderate attentional executive dysfunction in the context of a good premorbid cognitive functionality (WAT: 33) was reported.
The neuropsychological assessment was carried out at baseline (Table 1). JC’s performance was compared with available age, education, and gender-matched normative data. The neuropsychological assessment included the following measures: MMSE; Addenbrooke´s Cognitive examination [11]; Rey auditory verbal learning test [12]; Complex Rey Figure [12]; Semantic Fluency; Phonological Fluency; Trail making test Part A [13]; Trail making test Part B [13]; Digit span forward and backwards [14]; Wisconsin card sorting test [15].
| Neuropsychological assessment | Patient´s raw score | Patient´s Z score |
| ACE (max. 100) | 93 | |
| MMSE (max. 30) | 30 | |
| WAT | 33 | |
| Reasoning (WAIS) | 12 | |
| Ineco frontal screening (IFS) (max. 30) | 21 | |
| Phonological fluency | 10 | -1,18 |
| Semantic fluency | 15 | -1,27 |
| Forward digit span | 7 | 0,15 |
| Backward digit span | 4 | |
| Trail making A | 48 seconds | -2,14 |
| Trail making B | 81 seconds | -1,4 |
| Wisconsin card sorting test | 6/6 | |
| RAVLT immediate recall (max. 75) | 35 | -2,35 |
| RAVLT delayed recall (max. 15) | 5 | -2,54 |
| RAVLT recognition (max. 15) | 15 | -0,36 |
| Complex rey figure immediate (max. 36) | 34 | 0,18 |
| Complex rey figure delayed recall (max. 60) | 21 | -0,21 |
Beyond what has been shown, the patient presented a good cognitive performance, generally speaking. He was oriented in time and space, and he got normal results on general screening tests (ACE & MMSE). According to his background, the patient obtained descended values in executive screening test (INECO frontal screening), attentional alternation (Trail making test part B) and inhibitory control (short part of the Hayling test). He also presented with difficulties in memory tests related to attentional fluctuations and executive dysfunction, demonstrating problems in acquiring new information when more strategies were required, though he had storage and long-term evocation preserved (Rey auditory verbal learning test).
Functional profile at treatment initiation
An occupational therapy assessment was also done, in which Mr. JC presented an independent performance in basic activities of daily life (FIM: 122/126) [10, 11] and in instrumental ADL (Lawton & Brody: 7/8) [12], requiring help to do the household cleaning and to organize his daily environment.
Regarding his daily routine, the patient was studying Biodiversity Handling, Management and Conservation in CAECE University. Structured activities were only observed within his University occupation. However, a lack of participation in physical and recreational activities was evident, requiring a better occupational balance in his daily routine. Moreover, JC has decreased his participation in social activities, and his friendships deteriorated following the accident as well.
From a mood point of view, Mr. JC showed moderate to severe symptoms (BDI II: 21). Even though specific measures have not been administered, JC´s clinical records reported fatigue when more challenging activities took place, whether within cognitive or higher time requirements.
Initial intervention
Once the initial assessments had been performed, the patient started an interdisciplinary cognitive rehabilitation program which included sessions of study methodology, occupational therapy (OT), music therapy and neuropsychiatry interviews.
Due to the impairments described above, the first OT interventions were initially oriented towards acquiring a better organisation in his home and an adequate occupational balance through the different activities was pursued. Once this initial objective was accomplished, the specific work integration program, that is about to be described, was designed [13].
Specific work integration programTop
Program description
In tandem with the treatment Mr JC was already undergoing, it was suggested that the patient do a specific work integration program. At the start, Mr. JC did an initial interview with an expert occupational therapist (AC), in which the need to go through the following stages was identified: vocational assessment, look for work stations, preparation for job interviews and training in a real work station.
Stage 1: Vocational assessment
Within one OT session, the previous educational and work experience is explored together with the patient`s vocational interests and capacities. The assessment is performed through the application of specific and previously structured questionnaires, which are tailored according to the patient’s needs and abilities.
In the same interview, the work field of his career was identified as including being a ranger, the study of animals, insects or weather changes and generalities of the environment. A main interest in the countryside was found, where he could be next to flora and fauna.
Stage 2: Looking for work stations
Over the course of 3 OT sessions, possible work stations are identified. The patient writes down a list of different places and their contacts (email, phone number, their name), that are related with the person´s studies. The patient should bring a table with all the places written down. It is important that the person does this task at home, in order to train for responsibilities related to duties, required for every job. In the following session, the patient and the OT contacted those places. In the third session, all the responses are analysed, writing pros and cons about each work station.
In the first session, different work stations in the City of Buenos Aires were identified: Ecological reserve, zoos, natural parks and vets. Mr. JC wrote down the places in his email. While exploring the different tasks that could be performed in those places, the Vet was selected on the basis that it offers a structured environment and an appropriate framework with respect to the training that the patient required. In this context, the tasks involved in the job were tailored and simplified to suit Mr. JC’s post-trauma skills level.
In the next session, he brought a table with the information required; that is to say, all the names of the places, contact person, address, phone number and email address. Once that task was supervised, Mr. JC called the different places and wrote emails with his CV attached.
During the third session, the patient presented the same table with the answers included. He also opened his email and showed the replies he’d received. Some of those who responded said that they were not looking for volunteers, or that they did not have a place for practitioners at that time. In the end, there was only one possibility left, at a Vet close to his house.
During this stage, the patient revealed responsibility with the task he had to make at home. Even though, Mr. JC required constant OT suggestions, stimuli and prompts in order to complete the tasks in time.
Stage 3: Preparation for job interviews
The 3rd stage took place in 7 OT sessions. Modelling is done through applying filming and role playing techniques, in order to achieve an adequate performance in a job interview [14]. In one session, all the items related to social skills are presented and explained with practical examples. A brief role play is done, clarifying each social skill. The patient is asked to assist the following session as if he is going to a job interview and a video consent is signed. In the next session, the patient attends dressed formally and with the CV in his hands. The video recording is initiated while a simulation of the job interview takes place. The last session in this stage, consists in assessing the role play with a specific report of social skills for a job interview, which has been specially designed for the actual stage. It is completed by the patient and the professional while watching the video record in order to guarantee a level of adequate self-awareness [15].
In the 4th and 5th sessions, personalised training according to the results of the specific report of social skills implicated in a job interview (SRSSJI) takes place. That is, for example, if the patient presents a deficit in eye contact, then a role play, and other techniques, will take place emphasising that particular social skill in the context of a job interview. In the 6th session, a new simulation and video record of the job interview occur with a different interviewer, whom the person has not met yet. This is an important factor, because it is the closest it can get to a real Job Interview. Finally, in the 7th session, both the patient and the OT complete the SRSSJI again, while watching the video recording.
In this stage, a 10 point scale was designed contemplating the following items related to social skills: eye contact, voice volume, gestural expressions, interactive postures, corporal language, affective adaptation (emotional response), Active hearing and empathy, formal language and appropriate language, transmission of clear and relevant information, time devoted to the answers, respect time in the conversation and use of sense of humour.
This scale was completed by the OT and the patient self-assessment, in a scale that goes through 1, meaning complete absence and unsatisfactory performance of a certain skill and 10 represents complete presence and satisfactory performance according to the context suggested.
Stage 3 results
In the assessment which the patient completed, he registered a total score of 73/110. Showing principal difficulties related to social skills involved in a job interview, in the voice volume, transmission of clear and relevant information and eye contact.
The OT registered a total score of 68/110. The one reported descended numbers in the voice volume, gestural expressions, interactive postures, corporal language, affective adaptation (emotional response), Active hearing and empathy, formal language and appropriate language, transmission of clear and relevant information, time devoted to the answers, respect time in the conversation and eye contact. Regarding the last item, the patient used to look down at the floor or the desk in front of him. Occasionally, he drew a circle in the air with both eyes.
After the final stage of the program, and as to assess what has been trained, a second assessment was run with the same questionnaire. In this opportunity, the patient reported a score of 96/110. The OT registered a total score of 104/110. Mr. JC significantly improved his ability to make eye contact, gestural expressions, interactive postures, affective adaptation, active hearing and empathy, time devoted to the answers, respect time in the conversation. Mr. JC was appropriately smiling, listening to the questions, and he didn’t interrupt the interviewer as he did in the first assessment.
Stage 4: Training in a real work station
The patient has a job interview with his future supervisor where he can put into practice the skills previously trained. The training in a real work station has an initial length of 3 months. A gradual and progressive inclusion is advised, starting from 3 days a week, 4 hours each day. Also, an occupational therapist visits the work station twice a week, one hour each visit, with the objective of making interventions in situ. In the same time, the patient continues with his rehabilitation in the institute, where he can address the difficulties observed and shown in the training.
Once the first three stages were completed, and the “Vet assistant” was selected as the better work station to carry out the training, the patient and the OT localised 30 vets nearby the patient´s house in order to make a personal contact with each one of them. After the 30 vets in Belgrano´s town, in the capital city were identified, an agreement was elaborated in between of INECO foundation and the enterprise.
From all the Vets contacted, “Animal can” offered an interview with the occupational therapist responsible of the design of the actual program. After dispensing with all the legal issues and inquiries regarding Mr. JC, an interview between the patient and the supervisor was arranged.
Having had this interview, an agreement between the patient and the supervisor was finalised and we could then start the training. Both sides agreed that Mr. JC would assist for a period of 3 months, with the option of extending the training 3 more months if necessary, depending on the results of the assessments and wishes of both parties. Mr. JC assisted the Vet on Mondays, Wednesdays and Fridays from 9 till 1 pm.
Looking forward to support occupational interventions in the training program, the Vet provided a supervisor and an employee, who was a job partner. Both of them participated actively in the training process, through the performance report and having meetings with the occupational therapist. At the same time, the OT assisted twice a week, 1 hr each visit, throughout the whole program. Meanwhile, the patient continued with 2 OT sessions and 1 session of cognitive rehabilitation in the institute.
During the aforementioned stage, specific questionnaires were delivered at the start of the training and 3 months later. The same questionnaires were completed by Mr. JC., the occupational therapist, his work partner and the supervisor. The questionnaires implied specifically elaborated tests and work samples tailored to the “Vet assistant” work station. Through this method, certain objectives were established and interventions were carried out in order to improve the patient performance and participation along the process.
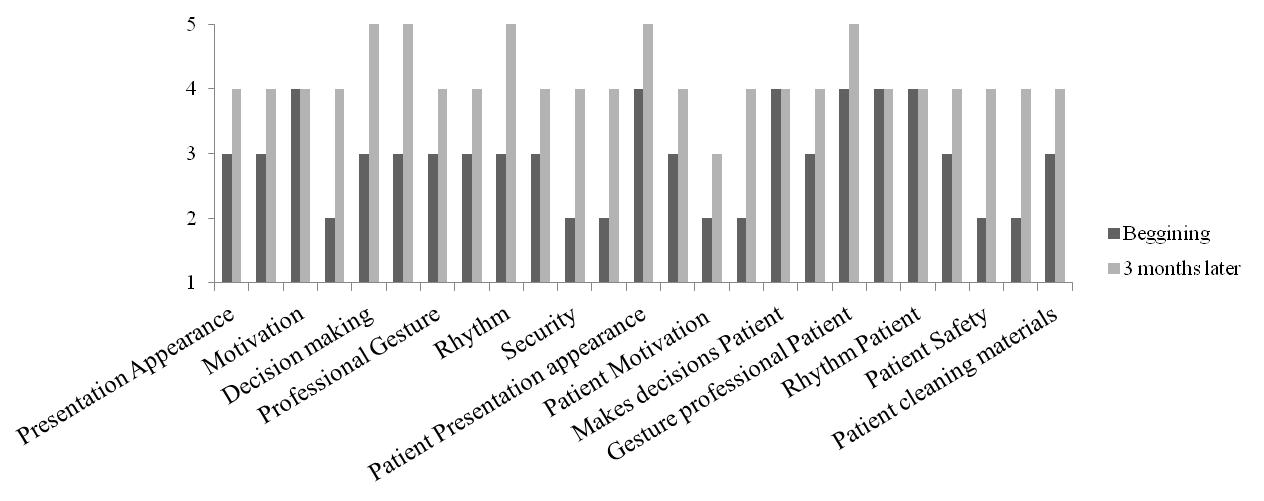
A work sample is a structured assessment, non-standardised, that is used in the framework of vocational rehabilitation in occupational therapy. It assesses basic habits, such as punctuality and appearance, and the organisation of one’s work and even, specific knowledge required for the job, for example, the ability to identify elements in this context and to make an adequate cleaning of the materials. It has a scale that goes from 1 to 5, 1 being a problematic area, regular capacity being 2 and an excellent ability in 5.
The work sample is divided into 4 parts: General characteristics, personality traits, work habits and specific knowledge. A job performance visual analogue scale (VAS) is established through these 4 themes, which were designed to be completed by both the supervisor and partner. In this case, the same was completed by the patient and the occupational therapist.
It was the responsibility of the supervisor to carry out the job performance VAS which was designed according to the real performance the patient showed and other important aspects involved in the worker’s role. In terms of judging the patient’s job performance, we focus on the assessment of the attendance (commitment in terms of punctuality and daily attendance) personal appearance, problem solving, pace maintenance during the shift, predisposition and the interest shown in the job, the task organisation, locating the necessary materials for the job and cleaning the tools and objects used. The graduation in this scale was from 1 to 10, meaning 1 an unsatisfactory performance and 10 a satisfactory performance on the work station. This questionnaire was completed by the supervisor at the beginning and at the end of the training.
The job performance VAS delivered was based in the report of the work habits JC had and specific knowledge needed according to the tasks performed. In this one, the graduation scale was of 4 points, where 3 represented a very good presence of work habits and 0 a total absence of those. The same graduation was taken to assess the specific knowledge. Mr. JC´s partner fulfilled this scale. Work habits assessed include: personal appearance, attendance, problem solving, task pace and supervision acceptance. Inside specific knowledge, we include the ability to find the materials, the materials order maintenance and the object´s cleaning.
In addition, a list of tasks performed helped in evaluating the employee’s performance through the analysis of the number of tasks that the patient incorporated over the course of the training. From the start of the programme, the tasks that Mr. JC performed were limited. The selected tasks were general cleaning, conditioning cages and animal feeding. The patient was responsible for certain tasks, that were performed in a routine way, while others were occasionally performed, varying according to the demands of each day.
As has been mentioned previously, OT sessions were carried out in this stage in the Vet and in the office. During the sessions in the patient´s work station, task performance was filmed, specific interventions were done in order to improve the general performance and conversations with his partner and supervisor were had so as to identify common mistakes and difficulties Mr. JC may have had. During the sessions carried out in the institute, routine tasks were registered, the filmed sessions were viewed in order to detect issues in his general functioning and strategies were planned in order to put them into practice later in the work station. In addition, a better context order was promoted, being the patient in charge of organising each space and distribute the materials in a functional way. Also, a social skills training was undertaken that was designed to target deficiencies that were observed in his work performance, for example, in the interaction and communication with his supervisor.
At the same time, gradual interventions in the work environment were done, modifying the requirements involved in the tasks that the patient had to perform, looking forward to promoting a gradual and progressive adaptation to the workplace.
Results of the training in a real work station
The work sample has been fulfilled by the patient and the OT. In the first assessment, Mr. JC reported a total score of 82/125. While the OT registered a score of 80/125.
Three months later, the scores improved to 102/125 (patient evaluation) and 105/125 (OT evaluation). These results reflect improvements in the presentation, appearance, communication with his partner and supervisor and supervision acceptance. Achievements were also found in the speed of decision taking, order, organization and routine pace. In addition, better results were found in security and professional attitude, understanding this one as a technical requirement to perform certain tasks, included in the work station. Figure 1 showing the scores at the beginning of the training and 3 months later.
Regarding the job performance VAS, which has been completed by his supervisor, a total score of 56/80 is reported. The same results were found at the end of the training.
In the last questionnaire, where work habits and specific knowledge has been reported, the first evaluation gave a total score of 29/36, achieving 2 more points by the end of the training (31/36). In this case, the patient´s capacity to find materials in the work place and problem solving have improved. However, Mr. JC did not get the highest score in both items. On the other hand, he did not improve in terms of his diligence when cleaning the materials, maintaining the same score. According to social interaction, the patient maintained the same good score, without changes.
In relation to the tasks performed, the patient increased his participation in those, doing new tasks as time went by, what represented a higher responsibility within the worker role. Mr. JC improved his participation and responsibility in the tasks required by the work station. The list of tasks performed showed that he performed 3 tasks when the training begun: general cleaning, cage conditioning and animal feeding. By the end of the stage, an increment up to 6 tasks has been observed. The 3 new tasks consisted on bathing dogs, organisation of the workplace and to be responsible for the Russian topos. This meant that he was completely in charge of feeding them (deciding what type of food he should choose), when and how much. He also had to maintain their habitat, with an adequate level of cleanliness and neatness.
Follow up
By the end of the first three months, the patient has shown improvements in the specific areas showed above. However, he expressed interest in developing another training program in a natural environment. For this reason an ecologic reserve was contacted and the work training program was repeated. This allowed the opportunity to maintain the achievements in a different workplace, providing a less structured framework, which represented a further challenge for the patient and, at the same time, was more motivating according to his interests. Having the opportunity to perform a new training program in the ecologic reserve, taking into considerations all the challenges it represented, was considered an important achievement by the rehabilitation team, the patient and his family. Mr. JC assisted at the ecologic reserve for a period of six months, on Tuesdays, Thursdays and Saturdays from 2 till 6 pm. The occupational therapist visited him at the workplace once a week. The same questionnaires were delivered, being completed by the patient, the professional, his work partners and supervisors. This second training session also afforded him the opportunity to continue improving his job performance, and enabled Mr. JC to demonstrate his competence while fulfilling the new job requirements.
By the end of the work integration program, thanks to the training stage, the patient was given the opportunity to attend to a job interview in a different park. Consequently, he obtained the job, which was according to his studies and area of interest in an ecological reserve. He still keeps that job, what had a major impact on his self-esteem. Moreover, he had the chance to build a relationship with his partners, going out together after work and celebrating their birthday parties as well. It was the first time JC could interact with others and build relationships after his accident.
DiscussionTop
Return to work is one of the main concerns within the rehabilitation of patients who had suffered a TBI. It depends on several aspects due to the complexity of the skills involved; and their interaction with the client´s impairment. Bonneterre (2013), Sjöström (2011) and Tyerman (2012) provided robust evidence of the importance that a personalized service delivery has in order to acquire a successful work integration. The present study adds the specificity and precision that a work integration program should have, describing each stage fully and deeply. We consider that the program can be replicated in different cultures tailoring the job performance assessments to each work station.
Alongside the present study, different stages of a return to work process in a patient with TBI have been described and put into practice: evaluation, look for work stations, preparation for job interviews and training in a real work station. In this particular case, the follow up could be done with the patient´s consent, if they preferred to continue with the training in a different environment. That is why six more months were carried on in an ecological reserve. Specific questionnaires were delivered in each stage, allowing data collection in order to validate the intervention effectiveness and giving the opportunity to detect problems in the work performance patients may have due to the several factors that interact after a TBI. Regarding the tasks performed, both a quantitative and qualitative improvement was found. As was proved by his independence in taking care of a specific type of animal, Mr. JC gained autonomy throughout the program.
There are several contextual issues that can affect the implementation of work integration programs as described in the present article. In this regard, it would be interesting to analyse how the economic and social context influenced a successful return to work program. In this particular case, Mr. JC had been looking for a suitable job for several years. When he finally got one, he lost it due to his impairments. After that experience, it was even more difficult to find a new opportunity. Furthermore, it is important to consider as well, the motivation the job seeker may have. Usually, people who have suffered from a brain injury and who are able to work, have a great desire to do so. Mr. JC always showed a high motivation to find and keep a job. This motivation allowed him to maintain the training, to perform tasks that were not to his liking and follow instructions from superiors, even when he did not agree with them. It is known that in rehabilitation, better results are obtained if the person is motivated with what they are doing. It would be possible to transfer this concept to a vocational rehabilitation process, suggesting that if the person is motivated to work, they will perform better than they would do without this motivation. It is also true that, even though professionals attempt to look for a job that accommodate the client’s interests, abilities and limitations, it is not always possible to get it, due to the range of job opportunities that are being offered at a particular time. In saying this, the job market may not have positions or jobs that would suit our client’s work profile and sometimes, they are not prepared to give the support that they would require. That is the reason why we support the idea of doing training in a workplace closest to the client´s ideal. This situation facilitates a work environment in which it is possible to assess an objective job performance and to identify what strategies would improve that performance. That is a simple way to assess results and to keep on working in order to promote a better work integration of people who have suffered a TBI. In this particular case, even if the position of Vet assistant was not ideal for Mr JC, it allowed him to get the required competences and skills to perform efficiently in a less structured position such as a workplace on an ecological reserve. In addition, this training gave him the abilities and experience to get a formal position of guide and park keeper, in a different reserve.
That being said, a specific work training program allows continuing the rehabilitation after a brain injury in an ecological context as a real workplace can be. Through this, the particular and specific difficulties that appear when performing a worker role can be addressed.
ConclusionTop
The present work integration program represents a successful approach for patients with cognitive deficits after a brain injury. We believe that the program methodology described in this case can be replicable in different contexts with patients that had suffered a brain injury and present cognitive deficits. However, future studies should replicate the present results, both using case report methodologies and group studies. It is also important to continue studying possible features towards a better work integration.
Conflicts of interest
The authors declare no conflicts of interest.
ReferencesTop
[1]Thornhill S, Teasdale GM, Murray GD, McEwen J, Roy CW, et al. Disability in young people and adults one year after head injury: prospective cohort study. BMJ. 2000; 320(7250):1631–1635.Article Pubmed
[2]Scottish intercollegiate guidelines network (SIGN). Brain injury rehabilitation in adults (SIGN publication no. 130) 2013.Article
[3]Kirsh B, Stergiou-Kita M, Gewurtz R, Dawson D, Krupa T, et al. From margins to mainstream: what do we know about work integration for persons with brain injury, mental illness and intellectual disability? Work. 2009; 32(4):391–405.Article Pubmed
[4]Benedictus MR, Spikman JM, van der Naalt J. Cognitive and behavioural impairment in traumatic brain injury related to outcome and return to work. Arch Phys Med Rehabil. 2010; 91(91):1436–1441.Article Pubmed
[5]Doig E, Fleming J, Cornwell PL, Kuipers P. Qualitative exploration of a client-centered, goal-directed approach to community-based occupational therapy for adults with traumatic brain injury. Am J Occup Ther. 2009; 63(5):559–568.Article Pubmed
[6]Sjöström R, Melin-Johansson C, Asplund R, Alricsson M. Barriers to and possibilities of returning to work after a multidisciplinary rehabilitation programme. A qualitative interview study. 2011; 39(3):243–250.Article Pubmed
[7]Tyerman A. Vocational rehabilitation after traumatic brain injury: models and services. Neuro Rehabilitation. 2012; 31(1):51–62.Article Pubmed
[8]Schönberger M, Ponsford J, Olver J, Ponsford M, Wirtz M. Prediction of functional and employment outcome 1 year after traumatic brain injury: a structural equation modeling approach. J Neurol Neurosurg Psychiatry. 2011; 82(8):936–941.Article Pubmed
[9]Bonneterre V, Pérennou D, Trovatello V, Mignot N, Segal P, et al. Interest of workplace support for returning to work after a traumatic brain injury: a retrospective study. Ann Phys Rehabil Med. 2013; 56(9–10):652–662.Article Pubmed
[10]Reith FCM, Van den Brande R, Synnot A, Gruen R, Maas AI. The reliability of the Glasgow Coma Scale: a systematic review. Intensive Care Med. 2016; 42(1):3–15.Article Pubmed
[11]Mathuranath PS, Nestor PJ, Berrios GE, Rakowicz W, Hodges JR. A brief cognitive test battery to differentiate Alzheimer's disease and frontotemporal dementia. Neurology. 2000; 55(11):1613–1620.Article Pubmed
[12]Rey A. Psychological examination of traumatic encephalopathy. Archives de Psychologie. 1941. 28:286–340. [Sections translated by J. Corwin, & F. W. Bylsma, The Clinical Neuropsychologist, 1993; 4–9. Complex Rey Figure (Rey, 1949)].
[13]Partington JE, Leiter RG. Partington’s pathway test. Psychological Service Center Bulletin, 1949; 1:9–20.
[14]Wechsler D. Wechsler adult intelligence scale – III. New York: Psychological Corporation. 1991.
[15]Grant DA, Berg EA. A behavioral analysis of the degree of reinforcement and ease of shifting to new responses in a Weigl-type card sorting problem. Journal of Experimental Psychology. 1948; 38(4):404–411.Pubmed
[16]Hall KM, Mann N, High WM, Wright J, Kreutzer JS, et al. Functional measures after traumatic brain injury: ceiling effects of FlM, FIMFAM, DRS, and CIQ. J Head Trauma Rehabil. 1996; 11(5):27–39.Article
[17]Hamilton BB, Laughlin JA, Granger CV, Kayton RM. Interrater agreement of the seven-level Functional Independence Measure (FIM). Arch Phys Med Rehabil. 1991; 72(10):790.Article
[18]Vergara I, Bilbao A, Orive M, Garcia-Gutierrez S, Navarro G, et al. Validation of the Spanish version of the Lawton IADL Scale for its application in elderly people. Health and Quality of Life Outcomes. 2012; 10:130.Article Pubmed
[19]American Occupational Therapy Association. Occupational therapy practice framework: Domain and process (2nd ed.). 2008; 62(6):625–688.Article
[20]Bell MD, Weinstein A. Simulated job interview skill training for people with psychiatric disability: feasibility and tolerability of virtual reality training. Schizophr Bull. 2011; 37(Suppl 2):S91–97.Article Pubmed
[21]Goverover Y, Johnston MV, Toglia J, Deluca J. Treatment to improve self-awareness in persons with acquired brain injury. Brain Inj. 2007; 21(9):913–923.Article Pubmed
 Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved