



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Cancer Research & Therapy
Volume 1, Issue 7, September 2013, Pages 186-193
Case reportOpen Access
Primary small cell neuroendocrine carcinoma of the breast: a report of two cases and review of the literature
-
Spinelli C1,
Fregoli L1,*
 ,
Biricotti M1,
Pucci V1,
Grosso M2,
Orsini F2,
Spisni R1,
Usolini C3 and
Caldarelli C4
,
Biricotti M1,
Pucci V1,
Grosso M2,
Orsini F2,
Spisni R1,
Usolini C3 and
Caldarelli C4
*Corresponding author: Dr. Lorenzo Fregoli, Department of Surgical, Molecular Pathology and Critical Area, University of Pisa, Pisa 56124, Italy, Tel.: +393 47 8684438. E-mail: lorenzofregoli@gmail.com
Received 23 May 2013 Revised 4 August 2013 Accepted 12 August 2013 Published 20 August 2013
DOI: http://dx.doi.org/10.14312/2052-4994.2013-28
Copyright: © 2013 Spinelli C, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
Primary neuroendocrine carcinomas of the breast are extremely rare. Neuroendocrine tumors mainly occur in the broncopolmonary system and gastrointestinal tract. The diagnosis of small cell neuroendocrine carcinoma (SCNC) of the breast can only be made if a non mammary site is excluded or if an in situ component can be found. We are going to describe two cases and to discuss their clinical, radiological and pathological manifestations. Introduction: Neuroendocrine tumors are rare and slow-growing neoplasias derived from neuroendocrine cells. We describe two cases of small cell neuroendocrine carcinoma of the breast and discuss their clinical, radiological and pathological manifestations. Case report: Our patients are two Italian females (38 and 36 year-old) with no family history of breast disease. In both cases the diagnosis was confirmed after surgery, when immunohistochemistry revealed a neuroendocrine differentiation of the tumor. The patients are alive and disease free after more than ten years of follow-up. Conclusion: Primary neuroendocrine carcinomas of the breast are extremely rare. The diagnosis of SCNC of the breast can only be made if a non mammary site is excluded or if an in situ component can be found. After surgery, a strict follow-up including octreotide scan should be performed and this doesn’t differ from the one of the usual breast carcinoma.
Keywords: small cell neuroendocrine carcinoma; breast disease; scintigraphy; neuron-specific enolase (NSE); mammography
IntroductionTop
Neuroendocrine tumors are rare and slow-growing neoplasias derived from neuroendocrine cells, which are present throughout the body; they arise especially in the bronchopulmonary system but they have been described also in many extrapulmonary sites including gastrointestinal tract, prostate, bladder, ovary and cervices. Small cell neuroendocrine carcinoma (SCNC) of the breast is rare, accounting for less than 0.1% of all breast cancers and less than 1% of all neuroendocrine tumors [1, 2]. To our knowledge, only about 30 cases have been reported in the English literature since the first case reported in 1983 [3]. We present two cases of primary SCNC of the breast and discuss the clinical, radiological and pathological manifestation.
Case reportTop
Case one
A 38 year-old woman had presented for two months a painless mass in the right breast. Clinical investigation revealed no palpable axillary lymph nodes; she had no relevant past medical history and she had no familiarity for breast disease. The mammography revealed a circumscribed high-density lump in the lower external quadrant of the right breast (Figure 1). The ecography showed an irregular neoformation having both hypoechoic and hyperechoic components measuring about 2 cm. A fine-needle biopsy was performed and revealed a ductal carcinoma in situ with neuroendocrine aspect. An Octroscan scintigraphy showed a focal uptake in the right brest (Figure 2a).
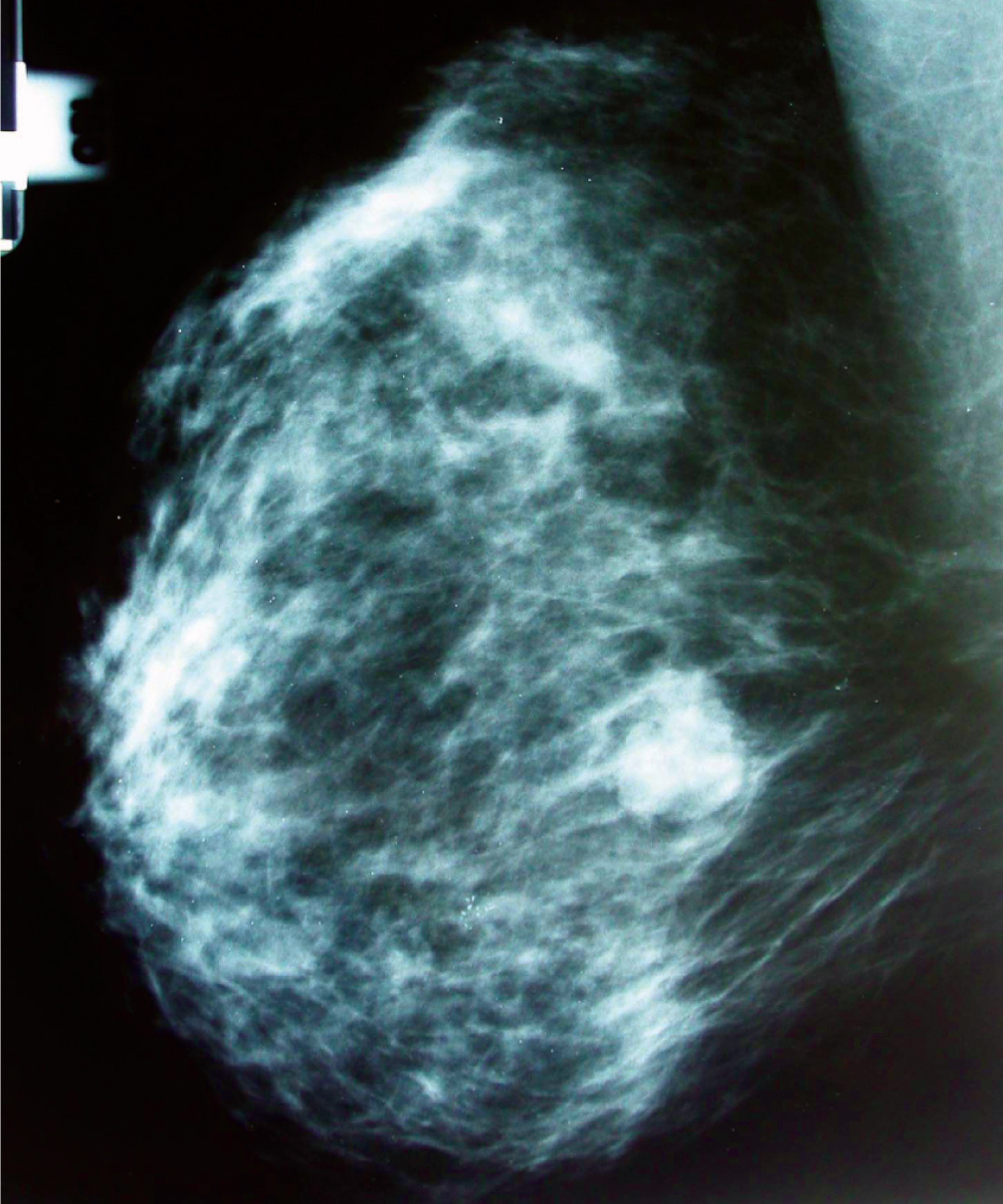
Figure 1 Mammography revealed a circumscribed high-density lump in the lower external quadrant of the right breast.
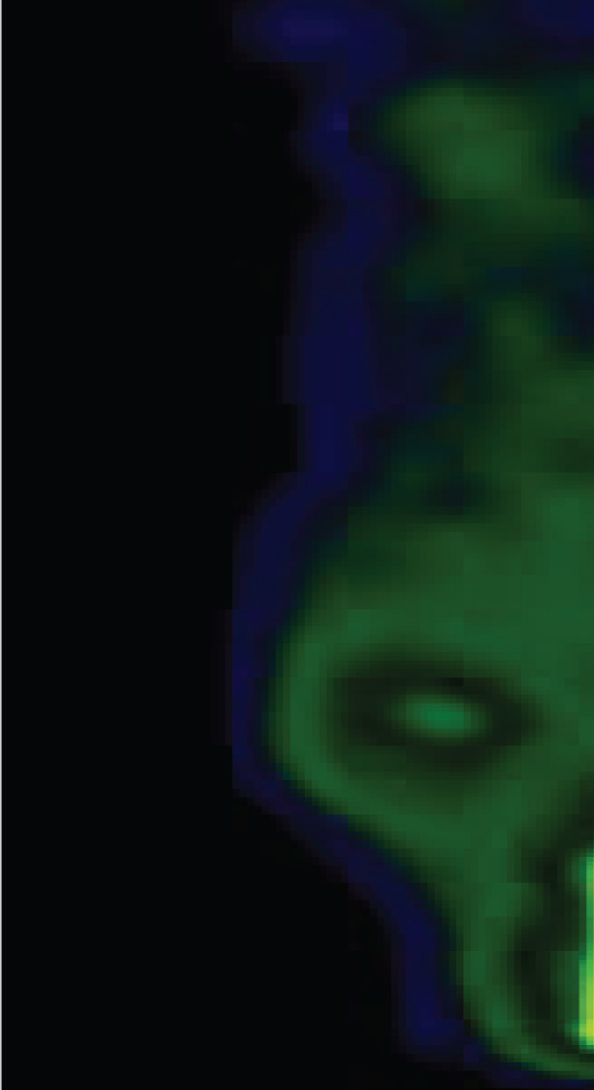
Figure 2a Octreoscan with 111-in-penteotride: the SPECT images showed a pathological focal uptake area in the right breast.
The patient had a quadrantectomy with right axillary nodes clearance. The resected mass was 8×4×3 cm with a tumor mass of 2.1×1.8 cm. The resection margins were clear. The histological examination showed that the tumor was an infiltrating ductal carcinoma with neuroendocrine differentiation (Figures 3a, 3b, 4, 5). The immunohistochemistry was positive for neuroendocrine differentiation markers including neuron specific enolase (NSE), chromogranin and synaptophysin in more than 90% of tumor cells. The estrogen receptor was positive in 90% and progesterone receptors in 20% of the tumor’s cells. Histological examination also showed that only 1 out of 16 lymph nodes were positive for metastases. The tumor stage was IIB. Additional chemotherapy, on the base of the current literature, was administrated with FEC and tamoxifen. After 12 years of follow-up with periodic mammography and octreotide scan (Figure 2b), the patient is disease free. Mammography of the right breast show a circumscribed, high density mass (Figure 1).
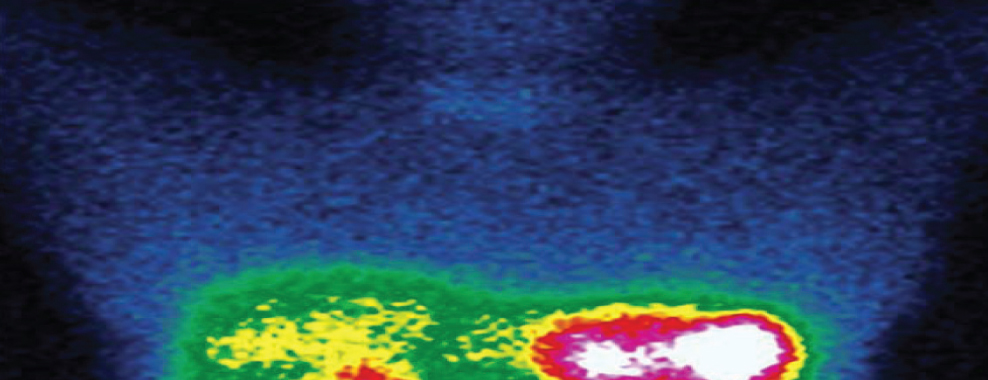
Figure 2b Octreoscan with 111-in-penteotride: planar image did not showed areas of pathological focal uptake.
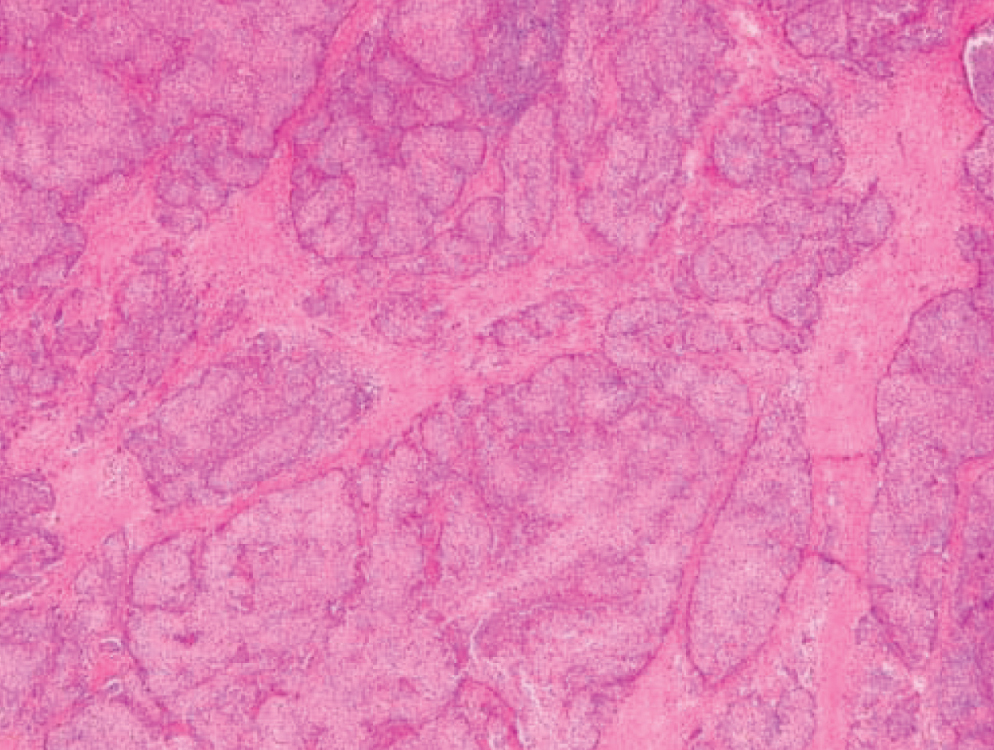
Figure 3a SCNC of the breast: haematoxylin and eosin.
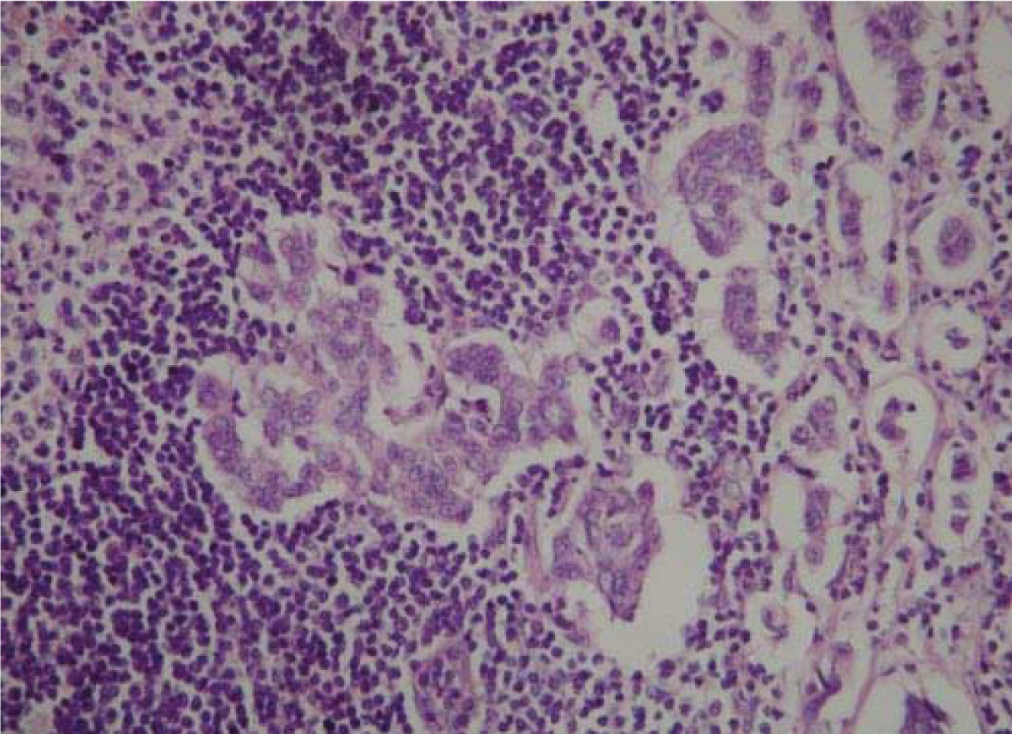
Figure 3b SCNC of the breast: metastatic lympho nodes.
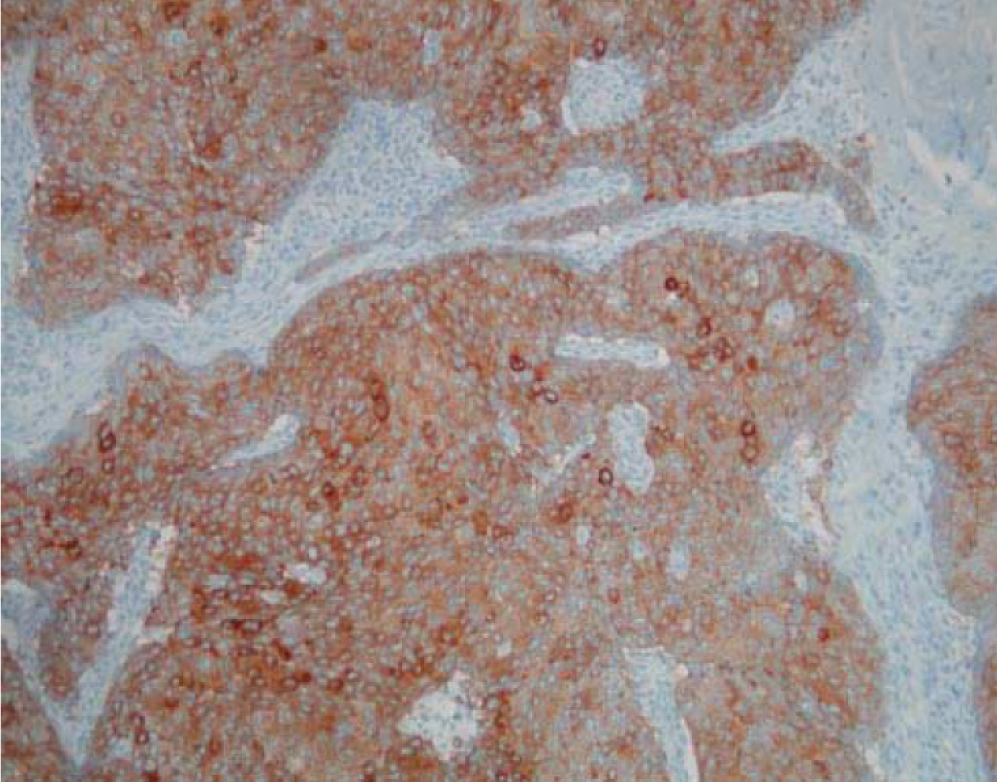
Figure 4 Section showing positive staining for synaptophysine.
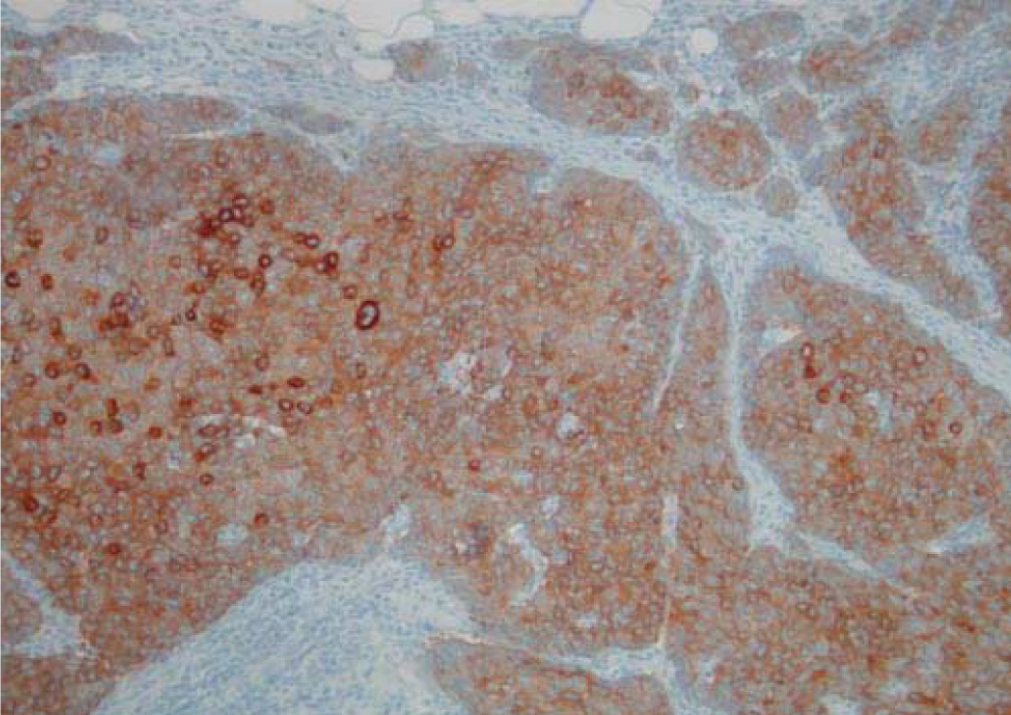
Figure 5 Histopathological findings reveal a neuroendocrine tumor.
Case two
A 36 year-old female patient with no family story for breast disease presented with a painless mass in the lower external quadrant of the left breast. There was no nipple retraction, dimpling or palpable axillary lymph nodes. The mammography revealed a roundish high density neoformation and the ecography showed a lump of 15 mm with an inhomogeneous central area (Figure 6).
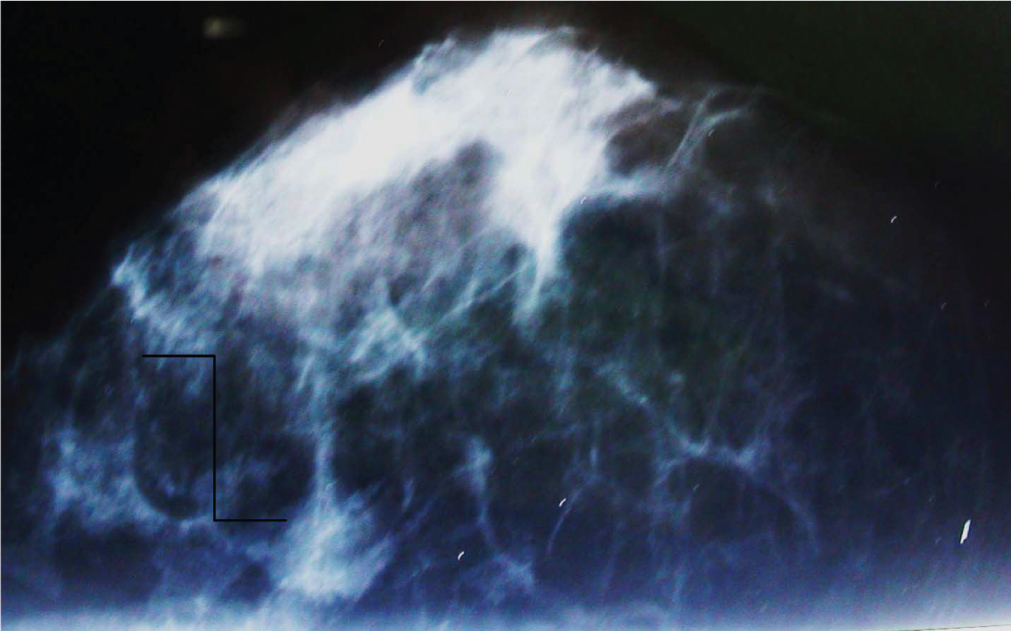
Figure 6 Mammography of the left breast reveal a roundish high density neoformation.
A quadrantectomy with left axillary nodes clearance was performed and the resected mass was 6×6×4 cm with a tumor mass of 17 mm. The anatomopathological examination revealed an infiltrating ductal carcinoma. Immunohistochemically, more than 90% of the tumor cells were positive for neuroendocrine differentiation markers, including synaptophysin, chromogranin and neuron specific enolase (NSE). The estrogen receptor was positive in 85% and progesterone receptors in 20% of the tumor’s cells. The resection margins were clear. There was no evidence of axillary lymph nodes metastases. The tumor stage was I. Any biopsy was performed prior to quadrantectomy, because of the high suspicion of malignancy showed by mammography. The patient was operated again after five years from the first surgery and a radical quadrantectomy and lymphadenectomy were performed. Definitive histology confirmed a small cells neuroendocrine tumor. The surgery was followed by adjuvant chemotherapy with CMF (cyclophosphamide, methotrexate and fluorouracil). After 10 years the patient is disease free.
Review of literature
We reviewed all the English literature on PubMed about the neuroendocrine carcinoma of the breast from 1983 to 2012, considering, for each article, the authors, the number of cases described (and for each case we considered the size of the tumor, the expression of estrogen receptors and the patient’s status at the end of the follow-up) and the year of publication. The cases described were 114, the median age was 57 years (range 28-87 years), the estrogen receptors were positive in the 50% of the cases (Table 1).
| Author | Number of cases | Year | Age | Size (cm) | ER | Status |
| Wade et al. [5] | 1 | 1983 | 52 | 10 | ns | DOD |
| Papotti et al. [6] | 3 | 1992 | 64 | 2 | neg | NED |
| 41 | 3.5 | neg | DOD | |||
| 69 | 5 | pos | DOD | |||
| Francois et al. [7] | 1 | 1995 | 68 | 4 | neg | DOD |
| Chua et al. [8] | 1 | 1997 | 45 | 4.5 | neg | NED |
| Fukunaga et al. [9] | 1 | 1998 | 56 | 10.5 | neg | NED |
| Yamasaki et al. [10] | 1 | 2000 | 41 | 4.5 | neg | NED |
| Shin et al. [11] | 10 | 2000 | 43 | 1.3 | ns | NED |
| 44 | 2 | ** | NED | |||
| 46 | 3.4 | ** | AWD | |||
| 50 | 2.2 | ** | NED | |||
| 51 | 1.5 | ** | NED | |||
| 57 | 2.5 | ** | NED | |||
| 62 | 5 | ** | AWD | |||
| 64 | 1.8 | ** | NED | |||
| 70 | 4 | ** | NED | |||
| 67 | 2 | neg | NED | |||
| Sridhar et al. [12] | 1 | 2004 | 58 | 2 | neg | NED |
| Jochems et al. [4] | 1 | 2004 | 71 | 3 | pos | NED |
| Bigotti et al. [13] | 1 | 2004 | - | 18 | neg | DOD |
| Adegbola et al. [2] | 3 | 2005 | 46 | 1 | neg | NED |
| 60 | 1.7 | neg | DOD | |||
| 61 | 1.7 | neg | AWD | |||
| Shaco-Levy R et al. [14] | 1 | 2007 | 28 | - | - | - |
| Kitakata et al. [3] | 1 | 2007 | 44 | 4.5 | neg | NED |
| Mirza et al. [15] | 1 | 2007 | - | - | - | - |
| Yaren et al. [16] | 1 | 2007 | 76 | 5 | pos | NED |
| Ogawa et al. [1] | 1 | 2008 | 34 | 2.7 | pos | NED |
| Sadanaga et al. [17] | 1 | 2008 | 33 | ns | neg | NED |
| Kinoshita et al. [18] | 1 | 2008 | 31 | 6 | neg | DOD |
| Haji et al. [19] | 1 | 2009 | 68 | 5.8×4.3 | neg | DOD |
| Yamaguchi et al. [20] | 1 | 2009 | 51 | 3 | neg | AWD |
| Ersahin et al. [21] | 2009 | |||||
| Ochsenreither et al. [22] | 1 | 2009 | 55 | ns | ns | NED |
| El Hassani et al. [23] | 1 | 2009 | 40 | 10 | neg | DOD |
| Stita et al. [24] | 1 | 2009 | 64 | 3×2 | pos | NED |
| Kawasaki et al. [25] | 32 | 2010 | 27-82 | - | - | - |
| Goucha et al. [26] | 1 | 2010 | 65 | 1.8 | pos | NED |
| Tajima et al. [27] | 17 | 2012 | 75 | ns | pos | |
| 67 | ns | pos | ||||
| 50 | ns | pos | ||||
| 25 | ns | pos | ||||
| 29 | ns | pos | ||||
| 66 | ns | pos | ||||
| 68 | ns | pos | ||||
| 73 | ns | pos | ||||
| 37 | ns | pos | ||||
| 38 | ns | pos | ||||
| 73 | ns | pos | ||||
| 46 | ns | pos | ||||
| 77 | ns | pos | ||||
| 70 | ns | pos | ||||
| 87 | ns | pos | ||||
| 83 | ns | pos | ||||
| 56 | ns | pos | ||||
| Wei et al. [28] | 74 | 2010 | 61.2 ± 12.4 | 2.70±2.06 | pos 70/74 | ns |
| Christie et al. [29] | 1 | 2010 | 64 | 4.5 | pos | ns |
| Richter-Ehrenstein et al. [30] | 9 | 2010 | 49-82 | 0.6-5 | pos (9) | ns |
| Latif et al. [31] | 1 | 2010 | 53 | 4.8×4.7 | neg | AWD |
| Lopez-Bonet et al. [32] | 8 | 2011 | ns | ns | pos (8) | ns |
| Nozoe et al. [33] | 1 | 2011 | 57 | 3 | pos | AWD |
| Cesaretti et al. [34] | 1 | 2011 | 68 | 2 | - | - |
| Kawanishi et al. [35] | 1 | 2011 | 67 | 0.8×0.7 | pos | NED |
| Saeed et al. [36] | 1 | 2011 | 60 | - | - | - |
| Singh et al. [37] | 1 | 2011 | 60 | 1.2 | pos | ns |
| Buttar et al. [38] | 1 | 2011 | 63 | ns | pos | AWD |
| Honami et al. [39] | 1 | 2011 | 54 | 0.5×1 | pos | NED |
| Jach et al. [40] | 1 | 2011 | - | - | - | - |
| Zhang et al. [41] | 1 | 2011 | 29 | 8.5×5.5 and 2 (2 masses) | pos | NED |
| An et al. [42] | 1 | 2012 | 64 | 0.8 | ns | ns |
| Righi et al. [43] | 105 | 2012 | 27-93 | ns | ns | ns |
| Alkaied et al. [44] | 1 | 2012 | 83 | ns | pos | AWD |
| Menéndez et al. [45] | 4 | 2012 | 44 | 2 | pos | NED |
| 68 | 3.6 | ns | NED | |||
| 58 | 1 | pos | AWD | |||
| 69 | 1 | pos | NED | |||
| Miura et al. [46] | 1 | 2012 | 72 | 1.5 and 0.3 (2 masses) | pos | ns |
| Wu et al. [47] | 13 | 2012 | 36-78 | 01-Apr | pos | ns |
| Sanguinetti et al. [48] | 1 | 2012 | 63 | 6,5 | ns | AWD |
| Yavas et al. [49] | 1 | 2012 | 77 | 3×2×2 | pos | NED |
| Ishida et al. [50] | 1 | 2012 | 37 | 3×2.5 | pos | NED |
| Boyd et al. [51] | 1 | 2012 | 50 | ns | pos | AWD |
| Yildirim et al. [52] | 6 | 2012 | 70 | 4.5 | pos | NED |
| 30 | 3.5 | neg | NED | |||
| 74 | 4 | pos | NED | |||
| 40 | 4.5 | pos | NED | |||
| 75 | 4 | pos | NED | |||
| 35 | 2 | pos | AWD | |||
| Graça et al. [53] | 1 | 2012 | 83 | 2.4 | ns | NED |
| Psoma et al. [54] | 1 | 2012 | 46 | 6.5 | ns | NED |
| Spinelli et al. [Present article] | 1 | 2012 | 38 | 2.1 | Pos | NED |
| 1 | 36 | 1.7 | pos | NED | ||
DiscussionTop
Neuroendocrine tumors of the breast are rare, accounting for less than 0.1 % of all breast cancer and less than 1% of all neuroendocrine tumors [1]. The age of incidence reported in literature varies from 40 to 70 years, with higher incidence in women over 60 years (our cases are in an early age). SCNC may represent either metastatic or primary lesions and carcinoma of the breast can be diagnosed if the presence of a non mammary primary site can be ruled out clinically, or an in situ is detected histologically or both [3]. It is important to differentiate primary breast neuroendocrine tumor from metastatic disease of the breast because of the differences in treatment.
To exclude a primary lung tumor a thorax X-ray and ct should be performed. Primary locations such as pancreas, stomach and bowel are excluded by performing an abdomen ct. Furthermore an octreotide scan is helpful to identify other sites of endocrine tumors [4].
On mammography, unlike common breast carcinomas, which tend to have poorly defined margins and associated microcalcifications, neuroendocrine tumors may appear as sharply circumscribed masses and often mimic fibroadenomas, cystitis or intramammary lymph nodes [1]. However the radiological features are nonspecific, and a fine-needle aspiration or core-needle biopsy examination is necessary for the diagnosis. Obviously, care should be taken to not provoke a carcinoid crisis, which can result from compressing the breast during mammography and fine-needle biopsy examination [1].
The histogenesis is still unclear because the presence of neuroendocrine cells in normal breast has not been proved conclusively. It has been suggested that SNSC is a variant of metaplastic carcinoma arising from a lobular or ductal carcinoma [2]. However some believe that SCNC is a distinct type of breast carcinoma different from the usual type.
Histologically, SCNC is similar to those arising from other sites [3]. The tumor cells are small and round or oval, and have a large nuclear cytoplasmatic ratio. The nuclei are hypercromatic with inconspicuous or no nucleoli. There is usually a high mitotic count. The expression of neuroendocrine markers by SNSC is very important [2]. Although some of these tumors are poorly differentiated, the positivity for neuroendocrine markers including synaptophysin, chromogranin and neuron specific enolase (NSE) will give strong support to the diagnosis, and this should be carefully searched for; both our cases were positive.
The prognostic relevance of neuroendocrine differentiation in breast carcinoma is a subject of debate. Although most studies reported an appreciably worse prognosis a few did not [2]. However the prognosis could be better in tumors detected at a smaller size, without lymph node involvement and with hormone sensitivity [17]. Finally a strict follow-up including mammography and octreotide scan should be performed to detect possible relapse or the arising of a carcinoma of the usual type, as showed by our case two.
ConclusionTop
Primary neuroendocrine carcinomas of the breast are extremely rare. The diagnosis of SCNC of the breast can only be made if a non mammary site is excluded or if an in situ component can be found. After surgery, a strict follow-up including octreotide scan should be performed and this doesn’t differ from the one of the usual breast carcinoma. On the base of current literature, the small cells neuroendocrine tumor of the breast does not differ, about the surgical approach, from the others histologies. Also for this rare tumor the estimated size by preoperative examinations play a critical role in the choice of surgical strategy, among more conservative or more radical operations. A special attention should by reserved for the regional lymphnodes, because these tumors frequently metastasize to that level, as we can infer from our literature review.
Conflict of interest
The authors wish to express that they have no conflict of interest.
ReferencesTop
[1] Ogawa H, Nishio A, Satake H, Naganawa S, Imai T, et al. (2008) Neuroendocrine tumor in the breast. Radiat Med 1:28-32. Article
[2] Adegbola T, Connolly CE, Mortimer G (2005) Small cell neuroendocrine carcinoma of the breast: a report of three cases and review of the literature. J Clin Pathol 58:775-778. Article Pubmed
[3] Kitakata H, Yasumoto K, Sudo Y, Minato H, Takahashi Y (2007) A case of primary small cell carcinoma of the breast. Breast Cancer 14:414-419. Article Pubmed
[4] Jochems L, Tjalma WA (2004) Primary small cell neuroendocrine tumour of the breast. Eur J Obstet Gynecol Reprod Biol 115:231-233. Article Pubmed
[5] Wade PM Jr, Mills SE, Read M, Cloud W, Lambert MJ (1983) Small cell neuroendocrine (oat cell) carcinoma of the breast. Cancer 52:121-125. Article Pubmed
[6] Papotti M, Gherardi G, Eusebi V, Pagani A, Bussolati G (1992) Primary oat cell (neuroendocrine) carcinoma of the breast. Report of four cases. Virchows Arch A Pathol Anat Histopathol 420:103-108. Article Pubmed
[7] Francois A, Chatikhine VA, Chevallier B, Ren GS, Berry M (1995) Neuroendocrine primary small cell carcinoma of the breast. Report of a case and review of the literature. Am J Clin Oncol 18:133-138. Pubmed
[8] Chua RS, Torno RB, Vuletin JC (1997) Fine needle aspiration cytology of small cell neuroendocrine carcinoma of the breast. A case report. Acta Cytol 41:1341-1344. Pubmed
[9] Fukunaga M (1998) Neuroendocrine carcinoma of the breast: a case report of pure type. APMIS 106:1095-1100. Article Pubmed
[10] Yamasaki T, Shimazaki H, Aida S, Tamai S, Tamaki K et al. (2000) Primary small cell (oat cell) carcinoma of the breast: report of a case and review of the literature. Pathol Int 50:914-918. Article Pubmed
[11] Shin SJ, DeLellis RA, Ying L, Rosen PP, Ying Liang BA, et al. (2000) Small cell carcinoma of the breast: a clinicopathologic and immunohistochemical study of nine patients. Am J Surg Pathol. 24:1231-1238. Article Pubmed
[12] Sridhar P, Matey P, Aluwihare N (2004) Primary carcinoma of breast with small-cell differentiation. Breast 13:149-151. Article Pubmed
[13] Bigotti G, Coli A, Butti A, del Vecchio M, Tartaglione R, et al. (2004) Primary small cell neuroendocrine carcinoma of the breast. J Exp Clin Cancer Res 23:691-696. Pubmed
[14] Shaco-Levy R, Dyomin V, Kachko L, Sion-Vardy N, Geffen DB, et al. (2007) Small cell carcinoma of the breast: case report. Eur J Gynaecol Oncol 28:142-144. Pubmed
[15] Mirza IA, Shahab N (2007) Small cell carcinoma of the breast. Semin Oncol 34:64-66. Article Pubmed
[16] Yaren A, Kelten C, Akbulut M, Teke Z, Duzcan E, et al. (2007) Primary neuroendocrine carcinoma of the breast: a case report. Tumori 93:496-498. Pubmed
[17] Sadanaga N, Okada S, Shiotani S, Morita M, Kakeji Y, et al. (2008) Clinical characteristics of small cell carcinoma of the breast. Oncol Rep 19:981-985. Article Pubmed
[18] Kinoshita S, Hirano A, Komine K, Kobayashi S, Kyoda S, et al. (2008) Primary small-cell neuroendocrine carcinoma of the breast: report of a case. Surg Today 38:734-8. Article Pubmed
[19] Haji AG, Sharma S, Vijaykumar DK, Mukherjee P, Babu RM, et al. (2009) Primary mammary small-cell carcinoma: A case report and review of the literature. Indian J Med Paediatr Oncol 30:31-34. Article Pubmed
[20] Yamaguchi R, Tanaka M, Otsuka H, Yamaguchi M, Kaneko Y, et al. (2009) Neuroendocrine small cell carcinoma of the breast: report of a case. Med Mol Morphol 42:58-61. Article Pubmed
[21] Ersahin C, Bandyopadhyay S, Bhargava R (2009 Thyroid transcription factor-1 and "basal marker"--expressing small cell carcinoma of the breast. Int J Surg Pathol 17:368-372. Article Pubmed
[22] Ochsenreither S, Marnitz-Schultze S, Schneider A, Koehler C, Daum S, et al. (2009) Extrapulmonary small cell carcinoma (EPSCC): 10 years' multi-disciplinary experience at Charité. Anticancer Res 29:3411-3415. Article Pubmed
[23] El Hassani LK, Bensouda Y, M'Rabti H, Boutayeb S, Kamouni M, et al. (2009) Primary neuroendocrine carcinoma of the breast, which chemotherapy? Indian J Cancer 46:352-354. Article Pubmed
[24] Stita W, Trabelsi A, Gharbi O, Mokni M, Korbi S (2009) Primary solid neuroendocrine carcinoma of the breast. Can J Surg 52:E289-90. Article Pubmed
[25] Kawasaki T, Nakamura S, Sakamoto G, Kondo T, Tsunoda-Shimizu H, et al. (2011) Neuroendocrine ductal carcinoma in situ of the breast: cytological features in 32 cases. Cytopathology 22:43-49. Article Pubmed
[26] Goucha A, Rekik W, Ben Mna N, Ben Hassouna J, Debbabi B, et al. (2010) Primary neuroendocrine carcinoma of the breast. Tunis Med 88:290-292. Article Pubmed
[27] Tajima S, Maeda I, Kanemaki Y, Nakajima Y, Tatsunami S, et al. (2010) Evaluation of CD56 and CD57 immunostainings for discrimination between endocrine ductal carcinoma in situ and intraductal papilloma. Pathol Int 60:459-465. Article Pubmed
[28] Wei B, Ding T, Xing Y, Wei W, Tian Z, et al. (2010) Invasive neuroendocrine carcinoma of the breast: a distinctive subtype of aggressive mammary carcinoma. Cancer 116:4463-4473. Article Pubmed
[29] Christie M, Chin-Lenn L, Watts MM, Tsui AE, Buchanan MR (2010) Primary small cell carcinoma of the breast with TTF-1 and neuroendocrine marker expressing carcinoma in situ. Int J Clin Exp Pathol 3:629-633. Article Pubmed
[30] Richter-Ehrenstein C, Arndt J, Buckendahl AC, Eucker J, Weichert W, et al. (2010) Solid neuroendocrine carcinomas of the breast: metastases or primary tumors? Breast Cancer Res Treat 124:413-417. Article Pubmed
[31] Latif N, Rosa M, Samian L, Rana F (2010) An unusual case of primary small cell neuroendocrine carcinoma of the breast. Breast J 16:647-651. Article Pubmed
[32] Lopez-Bonet E, Pérez-Martínez MC, Martin-Castillo B, Alonso-Ruano M, Tuca F, et al. (2011) Diagnostic utility of mammaglobin and GCDFP-15 in the identification of primary neuroendocrine carcinomas of the breast. Breast Cancer Res Treat 126:241-245. Article Pubmed
[33] Nozoe T, Sueishi K, Mori E, Iguchi T, Egashira A, et al. (2011) Primary neuroendocrine carcinoma of the breast: report of a case. Surg Today 41:829-831. Article Pubmed
[34] Cesaretti M, Guarnieri A, Gaggelli I, Tirone A, Francioli N, et al. (2011) Small cell carcinoma of the breast. Report of a case. Ann Ital Chir 82:61-64. Pubmed
[35] Kawanishi N, Norimatsu Y, Funakoshi M, Kamei T, Sonobe H, et al. (2011) Fine needle aspiration cytology of solid neuroendocrine carcinoma of the breast: a case report. Diagn Cytopathol 39:527-530. Article Pubmed
[36] Saeed A, Rehman A, Zaidi SA, Shaukat T, Jamil K, et al. (2011) Neuroendocrine carcinoma of breast. J Coll Physicians Surg Pak 21:371-373. Pubmed
[37] Singh S, Aggarwal G, Kataria SP, Kalra R, Duhan A, et al. (2011) Primary neuroendocrine carcinoma of breast. J Cytol 28:91–92. Article
[38] Buttar A, Mittal K, Khan A, Bathini V (2011) Effective role of hormonal therapy in metastatic primary neuroendocrine breast carcinoma. Clin Breast Cancer 11:342-5. Article Pubmed
[39] Honami H, Sotome K, Sakamoto G, Iri H, Tanaka Y, et al. (2011) Synchronous bilateral neuroendocrine ductal carcinoma in situ. Breast Cancer 1:342-345. Article Pubmed
[40] Jach R, Piskorz T, Przeszlakowski D, Huras H, Pitynski K, et al. (2011) Solid papillary carcinoma of the breast with neuroendocrine features in a pregnant woman: a case report. Neuro Endocrinol Lett 32:405-407. Pubmed
[41] Zhang JY, Chen WJ (2011) Bilateral primary breast neuroendocrine carcinoma in a young woman: report of a case. Surg Today 41:1575-1578. Article Pubmed
[42] An JK, Woo JJ, Kang JH, Kim EK (2012) Small-cell neuroendocrine carcinoma of the breast. J Korean Surg Soc 82:116-119. Article Pubmed
[43] Righi L, Rapa I, Votta A, Papotti M, Sapino A (2012) Human achaete-scute homolog-1 expression in neuroendocrine breast carcinoma. Virchows Arch 460:415-421. Article Pubmed
[44] Alkaied H, Harris K, Brenner A, Awasum M, Varma S (2012) Does hormonal therapy have a therapeutic role in metastatic primary small cell neuroendocrine breast carcinoma? Case report and literature review. Clin Breast Cancer 12:226-230. Article Pubmed
[45] Menéndez P, García E, Rabadán L, Pardo R, Padilla D (2012) Primary neuroendocrine breast carcinoma. Clin Breast Cancer 12:300-303. Article
[46] Miura K, Nasu H, Ogura H (2012) Double neuroendocrine ductal carcinomas in situ coexisting with a background of diffuse idiopathic neuroendocrine cell hyperplasia of breast: a case report and hypothesis of neuroendocrine tumor development. Pathol Int 62:331-334. Article Pubmed
[47] Wu J, Yang QX, Wu YP, Wang DL, Liu XW, et al. (2012) Solid neuroendocrine breast carcinoma: mammographic and sonographic features in thirteen cases. Chin J Cancer 31:549-556. Article Pubmed
[48] Sanguinetti A, Santoprete S, Lucchini R, Triola R, Loreti F, et al. (2012) A rare breast tumor: solid neuroendocrine carcinoma. Ann Ital Chir. Article
[49] Yavas G, Karabagli P, Araz M, Yavas C, Ata O, et al. (2012) HER-2 positive primary solid neuroendocrine carcinoma of the breast: a case report and review of the literature. Breast Cancer 1340-6868. Article Pubmed
[50] Ishida M, Umeda T, Abe H, Tani T, Okabe H (2012) Neuroendocrine carcinoma of the breast with a mucinous carcinoma component: A case report with review of the literature. Oncol Lett 4:29-32. Article Pubmed
[51] Boyd AS, Hayes BB (2012) Metastatic small cell neuroendocrine carcinoma of the breast. J Cutan Pathol 39:1042-1046. Article Pubmed
[52] Yildirim Y, Elagoz S, Koyuncu A, Aydin C, Karadayi K (2011) Management of neuroendocrine carcinomas of the breast: A rare entity. Oncol Lett 2:887-890. Article Pubmed
[53] Graça S, Esteves J, Costa S, Vale S, Maciel J (2012) Neuroendocrine breast cancer. Article Pubmed
[54] Psoma E, Nikolaidou O, Stavrogianni T, Mavromati A, Lytras K, et al. (2012) A rare case report of a primary large-cell neuroendocrine carcinoma of the breast with coexisting Paget disease. Clin Imaging 36:599-601. Article Pubmed
 Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved